1 Intro n anatomical landmark
advertisement

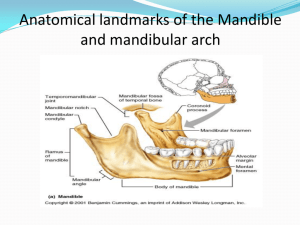
PRE-CLINICAL REMOVABLE PROSTHODONTICS INTRODUCTION AND ANATOMICAL LANDMARKS Dr. Tushar Bhagat 7508tvb@gmail.com Ref: Hasabulla Principal of complete denture. Course Description Course Code DSP 331 Course Name Preclinical Removable Prosthodontics Level Second Year (1st & 2nd Semester) Prerequisite none No. Of Credits 6 credits Credit Distribution 1 lecture + 1 practical Course Description References: 1. Hassaballa, M.H. and Talic, Y.F. Principles of Complete Denture Prosthodontics. 1st Edition. King Saud University-Academic Publishing and Press 2004. 2. Textbook of Complete Dentures. Rahn AO, Heartwell CM, 5th edition, 1992. 3. Dental Laboratory Procedures, Vol. 1 (Complete Dentures), Rudd and Morrow, 2nd Edition, 1986, The C.V. Mosby Co., St. Loius. Outcomes of this course Complete removable denture philosophies. Use of Articulators Occlusal contacts and teeth arrangement Laboratory procedure for removable prosthodontics Practical Sessions How to Perform labortary steps for removable prosthesis procedures. How to arrange artificial teeth for complete denture How to do surveying for RPD designing. RPD designing Methods of Assessment Continuous Assessment: 60% 1st Mid-term theory exam = 10% 2nd Mid-term theory exam = 10% 3rd Mid-term theory exam = 10% 1st Practical Assessment Examination = 05% 2nd Practical Assessment Examination = 05% 3rd Practical Assessment Examination = 10% Final Examination: 40% 5th Practical Assessment Examination = 10% 4th Mid-term theory examination = 10% Quizzes = 10% Logbook evaluation = 05% Attendance = 05% 60% 40% DEFINITIONS Prosthesis : an appliance which replace lost or congenitally missing tissues. Prosthetics : is an art and science of designing and fitting artificial substitute to replace lost or missing tissue. DEFINITIONS Dentulous ?? Edentulous?? OBJECTIVES OF COMPLETE DENTURE 1) To provide adequate masticatory function. 2) To restore natural appearance 3) To restore normal speech Anatomical landmark According to the clinical significance Landmarks of edentulous jaws Limiting structures Supporting structures Relief areas Limiting structures in maxilla Labial frenum-Fibrous band covered by mucous membrane. A labial notch is be narrow but deep enough in CD to avoid interference. Labial vestibule (sulcus)- bounded on one side by the teeth, gingiva and residual alveolar ridge and on the outer side by lips. Buccal frenum-Attachment of following muscles;levator anguli oris,orbicularis oris,buccinator. Buccal vestibule (sulcus)-Extends from buccal frenum anteriorly to the hamular notch posteriorly.The size of the vestibule is dependant uponcontraction of buccinator muscle position of the mandible masseter action amount of bone loss Hamular notch-It is depression situated between the maxillary tuberosity and the hamulus of the pterygoid plate .It is a soft area of loose connective tissue. The posterior extent of the denture in this region should end in the hamular notch ·Posterior palatal seal area[post dam]Soft tissue at or along the junction of the soft and hard palate on which the pressure within the physiological limits of the tissue can be applied by a denture to aid in the retention of the denture Made of two regions·→ 1.Pterygomaxillary seal-The part of the posterior palatal seal that extends across the hamular notch.It extends 3-4 mm anterolaterally to end in the mucogingival junction on the posterior part of the maxillary ridge. 2.Posterior palatal seal-This is a part of the posterior palatal seal area that extends between the two maxillary tuberosity Vibrating line(area)-An imaginary line drawn across the palate when the patient says ‘ah’ extending from one hamular notch to the other hamular notch; lying usually 2mm in front of fovea palatinae. Functions of the posterior palatal seal Aids in retention Prevents food accumulation Compensation for polymerization shrinkage Reduces the tendency for gag reflex due to downward movement of the denture during incising Limiting structures in mandible Labial frenum-Fibrous band extending from the labial aspect of the residual alveolar ridge to the lip. It is an active frenum containing a band of the fibrous connective tissue the that helps in attachment of the orbicularis oris muscle It is quite sensitive too and hence denture should have an appropriate labial notch. Labial vestibule-Runs from the labial frenum to the buccal frenum on each side. Mentalis muscle is quite active in this region Buccal frenum Buccal vestibule- Extends posteriorly from the buccal frenum to outside back corner of the retromolar pad Impression is widest in this region. . *Area maximisation can be safely done here as because the fibres of the buccinator runs parallel to the border and hence displacing action due to buccinator during its contraction is slight Lingual frenum-This area is shallow and hence should be recorded in function because at rest the height of the attachment is deceptive ;in fact in function it goes quite close to the crest of the ridge even though at rest it might be lower. Alveolingual sulcus-The space between the ridge and the tongue extending from the lingual frenum to the retromylohyoid curtain. A part of it is available for the lingual flange of the denture. It can be divided into three partsa.Anterior part or the pre mylohyoid region : Extends between the lingual frenum and pre mylohyoid fossa.It is the shallowest portion(least height) of the lingual flange. b.Middle region or the mylohyoid region:Extends from the premylohyoid fossa to the the distal end of the mylohyoid region. The denture border here should extend beyond and not below the mylohyoid ridge in this area if proper lingual seal is to be achieved. c.Posterior portion or Retromylohyoid fossa regionExtends from the end of the mylohyoid ridge end to the retromylohyoid curtain. Provides for a valuable undercut area so important retention in case of a mandibular denture. Retromylohyoid pad - Pear shaped triangular soft pad of tissue at the distal end of the lower ridge is referred to as the retro molar pad. Supporting structures Masticatory forces produce quite a pressure on the underlying structures and not everyplace beneath the denture can take such stress hence we need to know the areas which can bear the stresses well. These can be divided into- 1.Primary stress bearing area 2.Secondary stress bearing area Primary stress bearing area These are the areas that are most capable to take the masticatory load providing a proper support to the denture. Some desired properties for primary stress bearing area are- 1.Tightly adherent sufficient fibrous connective tissue with an overlying keratinized mucosa 2.Presence of cortical bone cover 3.Should be at right angles to the vertical occlusal forces. 4.No underlying structures should be present that will get harmed due to stress. Stress bearing areas in the maxilla Primary Posterolateral slope of the hard palate formed from the horizontal process of the palatine bone Posterolateral part of the residual alveolar ridge Secondary The palatal rugae areamucosal folds located in the anterior region of the palatal mucosa Maxillary tuberosity. Stress bearing areas in the mandible Primary- Buccal shelf area-area between the buccal frenum and the anterior border of the masseter Bounded medially by:crest of the ridge and by the retromolar pad * The total width of the bony foundation of this region becomes greater as the alveolar resorption continues Secondary residual alveolar ridge [the underlying bone is cancellous] Relief area These are the areas which either resorb under constant load or have fragile structures within or are covered by thin mucosa which can be easily traumatized & hence should be relieved. Relief areas in the maxilla Incisive papilla-Midline structure situated beneath the central incisors. It is an exit point of nasopalatine nerves and vessels It should be relieved failure of which would result in necrosis of the distributing areas and paresthesia of anterior palate. Mid palatine raphae-Median suture area covered by thin submucosa Relief is to be provided as it is supposed to be the most sensitive part of the palate to pressure Few areas like the cuspid eminence , fovea palatinae and torus palatinus may be relieved according to condition required Relief areas in the mandible Mylohyoid ridge-Running along the lingual surface of the mandible anteriorly the ridge lies close to the inferior border of the mandible while posteriorly it lies close to the ridge. The thin mucosa over the mylohyoid ridge may be traumatized and hence should be relieved. Also the extension of the lingual flange is to be beyond the palpable position of the mylohyoid ridge but not in the undercut Mental foramen-Lies on the external surface of the mandible in between the 1st and the second premolar region. It should be relieved specially in case it lies close to the residual alveolar ridge due to ridge resorption to prevent parasthesia Few places such as genial tubercle,torus mandibularis may be required to be relieved according to the condition. Other importance Many of the above landmarks help us in determining the original position of the teeth and thus helping us to set the teeth as they were within “the neutral zone” ; important for stability of the denture. Conclusion Thus, we see that a sound knowledge of the anatomical landmarks of the edentulous jaw is a prerequisite if one has to achieve the objective one has in mind; fabrication of a complete denture that has maximum retention, stability and support with preservation of underlying structures with minimum post insertion problems.