The Latest Clinical Application of Whole Genome Sequencing
advertisement

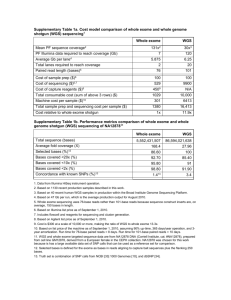
Current Perspectives: Clinical Applications For Whole Genome Sequencing Richard A. Leach, Ph.D. Vice President | Business Development | Complete Genomics Conflict of Interest Disclosure Vice President | Business Development Board Member | Stakeholder CME Learning Objectives 1. Understand the process of Whole Genome Sequencing (WGS) from tissue to data 2. Become familiar with relevant WGS quality metrics, genomic variants 3. Current perspective on clinical utility studies for WGS 4. Learn current and future clinical applications of WGS with some emphasis on preimplantation genetic diagnosis (PGD screening) and parental carrier screening 5. Clinical examples of WGS CME Learning Objectives 1. Understand the process of Whole Genome Sequencing (WGS) from tissue to data 2. Become familiar with relevant WGS quality metrics, genomic variants 3. Current perspective on clinical utility studies for WGS 4. Learn current and future clinical applications of WGS with some emphasis on preimplantation genetic diagnosis (PGD screening) and parental carrier screening 5. Clinical examples of WGS DNA Sequencing: Interrogating The 1° Structure Unknown Patient DNA Sequence 3’ – X X X X X X X X X X X X X X X X X X X X X X X X X X X X X 5’ – X Chain Termination AKA: Sanger Sequencing Known Patient DNA Sequence A T G C T T C G G C A A G A C T C A A A A A A T A Align & Compare “Call’ the Variant “Read” length ~700 bases Reference DNA Sequence C – 3’ T A T G C T T C G G C A T G A C T C A A A A A A T A C C G – 5’ Assign Variant Annotation & Interpret for Clinic DNA Sequencing: Genomic Variation Known Patient DNA Sequence A T G C T T C G G C A A G A C T C A A A A A A T A Align & Compare “Call’ the Variant “Read” length ~700 bases Reference DNA Sequence C – 3’ T A T G C T T C G G C A T G A C T C A A A A A A T A C C G – 5’ Genomic Variation = Different from Reference Genomic variants are either inherited or de novo • Single Nucleotide Polymorphism (SNP) • Tandem Repeats (STR, microsatellite) • Insertion • Deletion • Amplification • Inversion • Translocation • Aneuploidy Pathogenic? Next Generation Sequencing Next Generation = Massively Parallel PATIENT 5’- XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX - 3’ “Read” TGAACTAGTCTCGGA length 35-300 bases CGATGAACTAGTCTC CTCGGACCCGTAATG “Read Depth” TTTCGATGAACTAGT “Depth of Coverage” GACCCGTAATGGTCT ATTTCGATGAACTAG “Coverage” CTAGTCTCGGACCCG GTGCCATTTCGATGA “X-Fold Coverage” TCGATGAACTAGTCT ACTAGTCTCGGACCC GATGAACTAGTCTCG CCATTTCGATGAACT REFERENCE 5’- AGTGCCATTTCGATGAACATGTCTCGGACCCGTAATGGTCTCTTGGGTCTGAA - 3’ False Positive TAT Correct False Negative Call Rate & Accuracy Next Next Generation Sequencing Next Next Generation = Massively Parallel Massively Parallel Sanger Next Generation Highly Centralized Sequencing Factories -orHighly Distributed Desktop Sequencers Next Next Generation Genotyping: Known SNP’s & Microsatellites Targeted: Known finite regions Whole Exome: Coding region (~1% of total) • • Targeted Exome Capture (~180,000 exons) No non-coding DNA (i.e. no introns, regulatory regions, etc.) Whole Genome: Everything Next Next Gen Next Gen Microarray Sanger DNA Sequencing: Approaches to the Genome Process of Clinical Genome Sequencing PATIENT Results Delivery Sample Acquisition Report Generation Accessioning Genomic DNA Isolation Clinical Interpretation Data Packaging & Delivery gDNA Quality Control Variant Annotation Library Construction Variant Calling Sequencing Assembly Imaging Economics of Genome Sequencing Cost Per Genome $2MM 100,000 2003: $2,300,000,000 / 15 years 2014: $2,300 / 15 days 20K $350K Number of Whole Genomes Sequenced 1989 1 2 2003 2007 9 $5K 2011 $2.3K 2014 CME Learning Objectives 1. Understand the process of Whole Genome Sequencing (WGS) from tissue to data 2. Become familiar with relevant WGS quality metrics, genomic variants 3. Current perspective on clinical utility studies for WGS 4. Learn current and future clinical applications of WGS with some emphasis on preimplantation genetic diagnosis (PGD screening) and parental carrier screening 5. Clinical examples of WGS Moving WGS to the Clinic Many interwoven and complicated challenges for clinical adoption of WGS as standard of care WGS: Basic milestones for clinical adoption • Platform Validity • Proof of Clinical Utility • Health Economic Benefit WGS: Proving Clinical Utility “A test that is analytically sound but has no established clinical utility should not be offered Jennings, et al. Recommended Principles & Practices for Validating clinically.” Clinical Molecular Pathology Tests. Arch Pathol Lab Med. V133, May 2009 “…expresses- preferably in a quantitative formto what extent diagnostic testing improves health outcomes relative to the current best et al. Beyond Clinical Diagnostic Accuracy: The Clinical alternative.” Bossuyt, Utility of Diagnostic Tests. Clinical Chemistry- V58, December 2012 Clinical Utility Study Program • Global program of basic collaborative studies • Results published in leading clinical journals • 1° Goal: Compare diagnostic yield of WGS versus existing standard of care • 2° Goal: Demonstrate applications of WGS • 2° Goal: Study Health Economic Benefit WGS: Current Clinical Utility Studies 18 collaborative studies ongoing • Cardiology • Congenital Malformation • Developmental Delay / Intellectual Disability • Health Economics • Neurology • Newborn Screening • Oncology • Ophthalmology • Pathology Clinical Utility Study Program Oncology: Oxford Weatherall Institute • Prof. Ahmed Ashour Ahmed UK • Intra-operative monitoring of High Grade Serous Ovarian Cancer • Multiple fine-needle biopsies from a single tumor before and after chemotherapy • Used CGI Long Fragment Read Technology* • Study completed, manuscript submitted *Peters & Drmanac, et al. Nature, Vol. 487, July 2012 Epilepsy: UCL / NHS UK • Large Epilepsy study – hundreds of genomes • Brain surgery is current standard of care for certain debilitating epilepsies • Utility of WGS for surgical outcome prediction ASD / DDID / Malformation Canada • Diagnostic yield of WGS vs. clinical microarray • Prospective study: clinical assay performed in parallel with WGS • Assessing frequency of medically actionable variants unrelated to 1° reason for testing • Initial results very exciting Intellectual Disability: RUNMC • Prof. Han Brunner, Prof. Joris Veltman • Severe ID usually due to de novo variation • Diagnostic Yield of WGS vs. exome • Previous exome study published in NEJM • Current study 50 exome negative trios • Variants in exome & regulatory regions • Focus on de novo events Netherlands 2012: Diagnostic Exome 100 ID Trios All negative by Sanger, Microarray POSITIVE DIAGNOSIS NUMBER OF PATIENTS (n=100) All Mutations 16 De Novo Mutations 13 Autosomal Dominant 10 Autosomal Recessive 1 X-Linked 2 Inherited Mutations 16% Diagnostic Yield 3 Autosomal Dominant 0 Autosomal Recessive 0 X-Linked 3 Candidate Causal Variants 19 No Diagnosis 65 De Ligt, et al. New Engl J Med. Vol 367, November 2012 Netherlands 2013: Whole Genome 50 ID trios All negative by Sanger, Microarray, Exome POSITIVE DIAGNOSIS NUMBER OF PATIENTS (n=50) All Mutations 19 De Novo Mutations 18 Autosomal Dominant 14 Autosomal Recessive 0 X-Linked 4 Inherited Mutations 1 Autosomal Dominant 0 Autosomal Recessive 1 X-Linked 0 Candidate Causal Variants 8 No Diagnosis 23 38% Diagnostic Yield Netherlands Evolution of Diagnostic Yield for ID Netherlands 2005 Karyotyping Karyotyping Sanger Sequencing Sanger Sequencing Clinical Microarray Clinical Microarray Exome Sequencing Karyotyping Exome Sequencing Genome Sequencing Sanger Sequencing Genome Sequencing No Diagnosis Clinical Microarray No Diagnosis 2010 Exome Sequencing Genome Sequencing No Diagnosis 2013 Karyotyping Karyotyping Sanger Sequencing Sanger Sequencing Clinical Microarray Clinical Microarray Exome Sequencing 2015 Exome Sequencing Genome Sequencing Genome Sequencing No Diagnosis No Diagnosis CME Learning Objectives 1. Understand the process of Whole Genome Sequencing (WGS) from tissue to data 2. Become familiar with relevant WGS quality metrics, genomic variants 3. Current perspective on clinical utility studies for WGS 4. Learn current and future clinical applications of WGS with some emphasis on preimplantation genetic diagnosis (PGD screening) and parental carrier screening 5. Clinical examples of WGS Why do WGS for the clinic? To extend and improve the quality of human life. PERSONALIZED MEDICINE / PRECISION MEDICINE • Treatment focused • Uses panomics to select the right treatment for the right person at the right time. • Reactive Medicine P4 MEDICINE • Wellness focused • Personalized • Preventive • Predictive • Participatory • Proactive Medicine Pharmacogenomics • • • • • • Good Drug Antiplatelet CYP2C19 variant >15% non-metabolizers FDA black box warning ~$1BB wasted per year Pharmacogenomics abacavir acenocoumarol acetaminophen allopurinol amitriptyline aripiprazole arsenic trioxide atomoxetine atorvastatin azathioprine boceprevir brentuximab vedotin capecitabine carbamazepine carisoprodol carvedilol celecoxib cetuximab cevimeline chloroquine cisplatin citalopram clobazam clomifene clomipramine clopidogrel clozapine codeine crizotinib dapsone dasatinib denileukin diftitox desipramine dextromethorphan diazepam doxepin drospirenone duloxetine eltrombopag erlotinib escitalopram esomeprazole ethinyl estradiol everolimus exemestane flecainide fluorouracil fluoxetine flurbiprofen fluvoxamine fulvestrant galantamine gefitinib glibenclamide gliclazide glimepiride haloperidol hormonal contraceptives hydralazine iloperidone imatinib imipramine indacaterol irinotecan isoniazid isosorbide dinitrate ivacaftor lansoprazole lapatinib letrozole maraviroc mercaptopurine methylene blue metoprolol mirtazapine moclobemide modafinil mycophenolic acid nalidixic acid nelfinavir nilotinib nitrofurantoin norfloxacin nortriptyline olanzapine omeprazole oxycodone panitumumab pantoprazole paroxetine peginterferon alfa-2b pegloticase perphenazine Pertuzumab phenprocoumon phenylacetic acid phenytoin pimozide prasugrel pravastatin primaquine probenecid propafenone propranolol protriptyline pyrazinamide quinidine rabeprazole rasburicase ribavirin rifampin risperidone sertraline simvastatin sodium benzoate sulfadiazine sulfamethoxazole sulfasalazine sulfisoxazole tacrolimus tamoxifen tegafur telaprevir terbinafine tetrabenazine thioguanine thioridazine ticagrelor timolol tiotropium tolbutamide tolterodine tositumomab tramadol trastuzumab trastuzumab emtansine tretinoin trimethoprim trimipramine valproic acid vemurafenib venlafaxine voriconazole warfarin zuclopenthixol Parental Screening / Family Planning Alpha-Thalassemia Beta-Thalassemia Bloom Syndrome Canavan Disease Cystic Fibrosis Familial Dysautonomia Current targeted screening will be replaced by whole genome screening. Familial Hyperinsulinism Fanconi Anemia Fragile X Syndrome Gaucher Disease (Type I) Glycogen Storage Disease 1A Joubert Syndrome 2 Lipoamide Dehydrogenase Deficiency Maple Syrup Urine Disease Mucopolipidosis IV Neiman Pick Type A Nemaline Myopathy Spinal Muscular Atrophy Tay-Sachs Disease Usher Syndrome Walker-Warburg Syndrome Pre-Symptomatic Diagnosis Richard A. Leach, Ph.D. Jeffrey Gulcher, M.D., Ph.D. Idiopathic Disease Resolution Nick Volker Jacob Mayer Dimmock Margolis Verbsky Worthey LFR: A Major Sequencing Advancement LFR: A Major Sequencing Advancement Long Fragment Read (LFR) • • • • • 10 cells starting material <600 errors per diploid genome Phased – 98% Identify de novo variants Parent of origin Current Perspectives: Clinical Applications For Whole Genome Sequencing Richard A. Leach, Ph.D. Vice President | Business Development | Complete Genomics