Medical History Form
advertisement

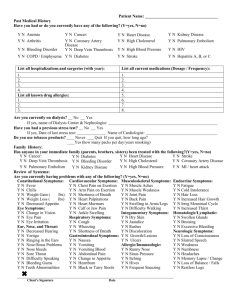
Name:_________________________ Age: _____________ Date: ___________________________ Who is your Primary Care Physician? _________________________________________________ What is the reason for your referral? __________________________________________________ Are you currently enrolled in a Hospice program or any type of Skilled Nursing Facility? ________ If so, please list the facility and the date you were enrolled. ________________________________ ________________________________________________________________________________ PLEASE CHECK IF YOU HAVE OR HAD ANY OF THE FOLLOWING: _____ Heart Attack _____ Heart Failure _____ Coronary Artery Disease _____ Coronary Angioplasty or Stent _____ Heart Murmur _____ Pacemaker _____ Stroke _____ High Blood Pressure _____ Infective Endocarditis _____ Blood Clots _____ Diabetes Mellitus _____ Shortness of Breath _____ Pneumonia _____ Sarcoidosis _____ Bleeding Problems _____ Bleeding Ulcers _____ Hiatal Hernia _____ Temporary Blindness _____ Varicose Veins _____ Kidney Failure _____ Difficulty Urinating _____ Weight Loss _____ HIV Positive _____ Heart Surgery _____ Angina/Chest Pain _____ Heart Catheterization _____ Echocardiogram _____ Childhood Heart Ailment _____ Valvular Heart Disease _____ Rheumatic Fever _____ Fainting/Dizzy Spells _____ Palpitations (heart racing _____ Leg Pain While Walking _____ Thyroid Problems _____ Asthma/Emphysema _____ Tuberculosis _____ Anxiety or Panic Attacks _____ Anemia _____ Leg/Ankle Swelling _____ Gallbladder Problems _____ Coughing Spells _____ Cancer _____ Kidney Stone/Infections _____ Aneurysm _____ Weight Gain _____ Hepatitis Do you have any other condition not listed above?_______________________________________ Do you Smoke? ____________________ How many packs per day? _______________________ For how many years? _______________ When did you quit? _____________________________ Do you use alcohol? ________________ How much? ____________________________________ Are you pregnant? __________________________________________________________________ List your allergies: __________________________________________________________________ Are you allergic to any of the following? ____X-ray or contrast dye ____ Iodine ____ Shrimp/Shellfish/Seafood ____ Local Anesthetics List your medications & doses:___________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________