RESULTS OF SELECTIVE USE OF MULTIMODALITY TREATMENT
advertisement

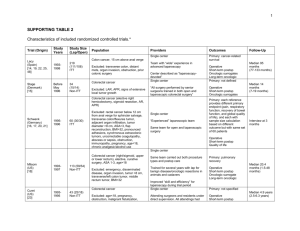
RESULTS OF SELECTIVE USE OF MULTIMODALITY TREATMENT IN ELDERLY PATIENTS WITH RECTAL CANCER. Faisal Elagili M.D.1, Luca Stocchi M.D.1, Kalady MF M.D.1,Abdel-Wahab M MD2, David W Dietz, M.D1 1:Department of Colorectal Surgery, Digestive Disease Institute, Cleveland Clinic, Cleveland/OH 2:Department of Radiation Oncology, Cleveland Clinic, Cleveland/OH Background: Chemoradiation followed by surgery is recommended for stage II- III rectal cancer and selectively used for stage IV. Elderly patients are less frequently offered multimodality therapy. The aims of our study were to assess the reasons for chemoradiotherapy omission and the oncologic outcomes of elderly patients with rectal cancer. Patients and methods: Patients≥ 70 years old with stage II-IV rectal cancer treated between 1990-2007 were identified from an institutional, IRB-approved cancer database and chart review. All patients underwent radical resection using total mesorectal excision principles. Patients receiving multimodality treatment were compared to patients undergoing surgery alone for clinic pathological variables, surgery type, postoperative morbidity and cancer outcomes. Results: 209 patients were identified (40% females, mean age 76 ±5) with a mean follow-up of 4.2 years, 104 of whom (49.8%) had surgery alone vs. 105 patients (50.2%) who received multimodality treatment. Patients receiving multimodality treatment were significantly younger (75 vs. 78 years, p=0.001) males (68% vs. 53%, p=0.03), with decreased Charlson Comorbidity Index score (3.1 vs. 4.0, p=0.005) and had greater proportion of stage III disease. Omission of chemoradiation was reportedly due to patient preference (n=12), previous pelvic radiotherapy (n=2), surgeon preference (n=58), and medical comorbidity (n= 32). Tumor grade, radial margin involvement, mean distance from the anal verge (7.5 vs 8.4 cm, p=0.17) rates of restorative procedures (57% vs. 64%, p=0.57) and postoperative morbidity were similar. Oncologic outcomes were similar including within individual disease stages (Table). Stage IV and poor tumor differentiation were factors independently associated with both OS and DSS, while age was independently associated with OS only and stage III disease with DSS only. Use of chemoradiotherapy was not independently associated with cancer outcomes. Conclusion: Selective omission of multimodality treatment in elderly patients in a single specialized unit was not associated with significant deterioration of oncologic outcomes with more advanced staging indirectly indicates the benefits. Table. Stage distribution, cancer outcomes and post op morbidity in patients treated with multimodality treatment vs. surgery alone. Multimodality Surgery alone P value treatment N=104 N=105 Tumor stage II 32 (30.5%) 55 (52.9%) 0.003 III 57 (54.3%) 34 (32.7%) IV 16 (15.2%) 15 (14.4%) Postoperative morbidity 37(35%) 25(25%) 0.12 5- year oncologic outcomes OS 44.3 % 47.4 % 0.86 DFS 40.1 % 45.5 % 0.79 DR 13 (12.4%) 14 (13.5%) 0.82 LR 5 (4.8%) 4 (3.8%) 1 DSS 63.5 % 68.1 % 0.49 OS: Overall survival, DFS: Disease-free survival, DR: Distant recurrence, LR: local recurrence, DSS: Disease-specific survival