jmri24853-sup-0001-suppinfo1
advertisement

1
Abbreviated Title Page
Title
Diffusion-weighted MR imaging does not reflect kidney fibrosis in a rat model of
fibrosis
2
ABSTRACT
Purpose: To assess apparent diffusion coefficient (ADC) derived from diffusionweighted (DW) magnetic resonance (MR) imaging as specific marker of renal fibrosis
in rats with unilateral ureteral obstruction (UUO).
Materials and Methods:
Thirteen rats were analyzed in group 1 (n=4), group 2 (n=3) and group 3 (n=6) and
measured using a clinical 3.0T MR scanner. Groups 1 and 2 were used to establish
the final imaging protocols for group 3. DW imaging with four b-values (0, 50, 300,
800 s/mm2) was conducted before UUO, at days 3 and 5 after UUO, after release of
the obstruction and after sacrifice. Renal cortical ADCs were correlated with
histological and ultrastructural analyses.
Results:
ADC values of group 3 are shown as mean ± standard deviation of [10-3mm2/s]. On
day 5, in vivo cortical ADC of obstructed fibrotic kidneys was significantly reduced
compared to unobstructed kidneys (1.4±0.086 vs. 1.535±0.087, p=0.0018). Post
mortem ADC dropped by 50 % and was significantly increased in obstructed vs.
unobstructed kidneys (0.711±0.094 vs. 0.566±0.049, p=0.0046). Histopathology of
obstructed kidneys showed tubular dilation, tubular cell atrophy and expansion of
interstitial space. Post mortem ADC correlated tightly with tubular lumen area (r=0.9,
p<0.001), fibronectin (r=0.8, p=0.003), collagen type I (r=0.73, p=0.007) and
interstitial expansion (r=0.69, p=0.013).
Conclusion:
. Compared to the in vivo measurements, post mortem renal ADCs were
considerably reduced and unlike in vivo, fibrotic kidneys exhibited consistently higher
3
ADC compared to healthy kidney parenchyma. Our data suggest that in vivo ADC is
unlikely to be a direct measure of renal fibrosis.
KEYWORDS: chronic kidney disease (CKD), renal fibrosis, diffusion-weighted (DW)
imaging, apparent diffusion coefficient (ADC), extracellular matrix, tubular dilation.
4
INTRODUCTION
The number of patients with chronic kidney disease (CKD), and ultimately with endstage renal disease, is steadily increasing (1, 2). The universal histological correlate
of CKD is renal fibrosis, a process characterized by replacement of functional renal
tissue by enhanced deposition of extracellular matrix (ECM) and activation and
expansion of interstitial fibroblasts (3). These changes are closely associated with
tubular atrophy, tubular dilation and interstitial mononuclear inflammatory cell
infiltrates. At present, renal biopsy is the only definitive method to assess renal
fibrosis. The lack of non-invasive markers or end-points for renal fibrosis in clinical
studies hinders the translation of novel treatment options, the identification of patients
with early fibrosis stages but also the possibility to closely monitor patients with CKD.
One non-invasive approach that was suggested to reflect renal fibrosis is diffusionweighted (DW) magnetic resonance (MR) imaging. This technique does not require
gadolinium contrast and is therefore particularly suited for patients with advanced
CKD. Since both random Brownian motion and directed water motion like renal
perfusion or tubular flow contribute to the DW signal decay, the apparent diffusion
coefficient (ADC) is higher in normal kidney than in other abdominal organs (4). A
number of clinical studies suggested that DW MR imaging might be a suitable
method to detect CKD (4-14). In a widely used animal model of renal fibrosis, the
unilateral ureteral obstruction (UUO), ADC was reduced in the obstructed murine
fibrotic kidneys compared to contralateral kidneys in vivo (10). It was suggested that
increased cellularity in this model is responsible for the decreased ADC. These
experimental data are in line with clinical studies showing lower ADC in patients with
CKD compared to controls without renal disease (7, 12, 13, 15).
Our aim was to establish imaging protocols for DW MR imaging in rats with UUO
5
using a clinical 3.0T MR scanner for routine monitoring of experimental fibrosis, to
introduce various control conditions to analyze in particular the contribution of renal
perfusion and function on ADC and to correlate the results with detailed
histopathological and ultrastructural analyses.
MATERIALS AND METHODS
Experimental Model and Design
The investigation was conducted according to the guidelines for studies using
laboratory animals (86/609/EEC), after approval by the local government authorities.
In total, this study included thirteen Male Wistar rats (Charles River, Erkrath,
Germany) weighing 275g ± 15g.
The rats were separated in three groups, where groups 1 (n=4) and 2 (n=3) were
used to develop the final protocol applied to group 3 (n=6). The rats were held in
rooms with constant temperature and humidity, 12h/12h light/dark cycle, with ad
libitum access to drinking water and food. Susceptibility artefacts observed in groups
1 and 2 were attributed to the fodder. Therefore, group 3 was deprived of fodder
eight hours before imaging receiving glucose water instead. All interventions and MR
imaging were performed under continuous Isoflurane (conc. 1.5%) anesthesia using
imaging protocols as described below.
After one week of acclimatization, all rats underwent baseline MR imaging five days
before the unilateral ureteral obstruction (UUO) was induced as described previously
(16). In short, under i.p. ketamin/xylazin anesthesia a median laparotomy was
performed and the left ureter was identified and ligated. The wound was sutured in
two layers. All rats were examined again with MR imaging three and five days after
6
UUO induction. No later time points were included because in this model renal
atrophy overrides active fibrogenesis at later stages. MR imaging on day 5 was
conducted before and after surgical release of the obstruction to analyze the effect of
large amounts of urine in the obstructed (hydronephrotic) kidneys on ADC. This
resulted in considerable changes in ADC values (Figure 1), and was therefore
performed in all groups. To remove the accumulated urine from the pelvis of fibrotic
kidneys, the abdomen was opened, the dilated ureter was dissected and the urine
was gently removed from the ureter and renal pelvis into the abdominal cavity.
Thereafter, the wound was closed by suture in one layer (the procedure took less
than 2 minutes). Group 2 underwent another MR examination 5 hours after release of
obstruction to investigate the effect of residual function of the fibrotic but no longer
obstructed kidney on ADC. Compared to measurement directly before obstruction
release, five hours later no major changes in both the renal DW MR signal and the
ADC were observed (data not shown). Therefore this measurement was not
performed in group 3. Finally, all rats were sacrificed by cervical dislocation and
immediately thereafter underwent a last MR examination. After post mortem MR
imaging, the obstructed and contralateral unobstructed kidneys were harvested,
weighed and processed for histological, immunohistochemical and biochemical
evaluation.
MR Imaging
Imaging was performed on a clinical 3.0T MR system (Achieva 3.0T TX, Philips
Healthcare) using a two-channel (Philips SENSE Flex M, Groups 1 & 2) and an eightchannel (Philips SENSE Wrist; Group 3) phased array surface coil according to a
protocol consisting of low resolution survey scan, coronal and transversal T2weighted (T2w) turbo spin-echo (TSE) images and transversal single-shot echo-
7
planar imaging (EPI) DW images with SPIR fat suppression and four b-values (0, 50,
300, 800 s/mm²) using the same sections as transversal T2w images to cover
identical anatomy. Introducing the eight-channel coil in group 3 allowed for
considerable improvements of the DW sequence (Supplementary Figure 1a-c):
smaller slice thickness, increased number of signals to reduce motion artefacts,
smaller EPI factor to reduce susceptibility artefacts and shorter echo time to increase
DW signal while measurement time could be basically maintained. More detailed
sequence parameters for group 3 are provided in Table 1. Further sequence
parameters for groups 1 and 2 can be found in the Supplementary Table 1.
MR Image Analysis
Kidney size was measured from cranial to caudal pole in the coronal T2w images by
two radiologists in consensus (M.P., 2 years of experience and F.S, 15 years of
experience). DW images were processed to compensate for motion using the
diffusion registration built into the MR scanner software. To measure renal ADC,
volumes-of-interest (VOIs) were placed by consensus of two radiologists (M.P. and
F.S.) in the renal cortex of both the obstructed and the contralateral kidney avoiding
susceptibility artefacts and displacement of the kidneys in different b-value
measurements. To this end, the DW images were overlaid with the transversal T2w
images for anatomical reference using the Imalytics Research Workstation (Philips
Technologie GmbH Innovative Technologies, Aachen, Germany). VOI contours were
manually drawn in cortical regions with good spatial correspondence between T2w
image and the DW images for all b-values. The DW images as well as binary masks
of the contours were exported to Matlab R2012b (MathWorks, Natick, MA, USA) for
ADC and intravoxel incoherent motion (IVIM) analysis. ADC maps were calculated by
voxel-wise linear regression analysis of the logarithmic DW images using a) all b-
8
values (ADCall), b) low b-values (0, 50, 300 s/mm², ADClo) and c) high b-values (300,
800 s/mm², ADChi). Perfusion fraction maps were determined by approximation
because the simultaneous nonlinear optimization of the four IVIM model parameters
can be compromised by noise and low number of sample points (17).
The IVIM model is given by (18):
𝑆(𝑏) = 𝑆0 ((1 − 𝑓)𝑒𝑥𝑝{−𝐷𝑏} + 𝑓𝑒𝑥𝑝{−𝐷∗ 𝑏})
[Eq. 1]
where D and D* are the true diffusion coefficient and pseudo-diffusion coefficient,
respectively, f is the perfusion fraction and S0 is the estimated signal intensity for
b=0. For high b-values, the pseudo-diffusion term becomes negligible and Eq. 1 is
well approximated by the mono-exponential ADC model (17, 18):
𝑆ℎ𝑖 (𝑏) = 𝑆0 (1 − 𝑓)𝑒𝑥𝑝{−𝐴𝐷𝐶ℎ𝑖 𝑏}
[Eq. 2]
where S0(1-f) is the intercept Shi(b=0) of the ADChi model and S0 can be
approximated by the intercept Slo(b=0) of the ADClo model. Mean ADC and mean
perfusion fraction were determined for the VOIs of obstructed and contralateral
kidney. The volume of the VOIs used for ADC and IVIM analysis was 15.9 ± 6.1 mm3
for the obstructed kidneys and 15.9 ± 4.7 mm3 for the contralateral kidneys.
Renal Morphology, Immunohistochemistry and Electron Microscopy
For the evaluation of renal histology and fibrosis, 2 μm sections of renal tissue, fixed
in methyl Carnoy’s solution and embedded in paraffin, were stained with periodic acid
Schiff’s (PAS). The indirect immunoperoxidase procedure to analyze fibrosis was
performed for α–smooth muscle actin (-SMA), collagen type I and fibronectin as
described previously (16, 19). All histological and immunohistochemical evaluations
were performed by a nephropathologist (P.B., 13 years of experience) in a blinded
manner. To evaluate the area stained by specific antibodies, computer-based
9
morphometry was performed as previously described (16, 19). In short, the area
positive for collagen I, fibronectin or α-SMA were quantified using the ImageJ
software (http://imagej.nih.gov/ij/). The expansion of interstitial space (tubulo-tubular
distance) was delineated manually in at least five cortical areas at 200x magnification
(approx. 60-80 measurements per rat per kidney). The tubular dilation was measured
by manually delineating the tubular lumen using “region of interest” (ROI) and
calculating the ROI area using the NDP.view software (Hamamatsu).
After approval by the local ethics committee, additional human PAS stained sections
acquired for diagnostic purposes were anonymously retrieved from the tissue bank of
the Institute of Pathology to take representative micrographs of kidney tissue with
and without fibrosis for the purpose of comparison.
For the analyses of ultrastructural changes in fibrosis (by P.B.), in particular the
tubular cell rarefication and expansion of interstitial space, transmission electron
microscopy was performed as described previously (20).
Statistical Analysis
If not denoted otherwise, all shown data and statistical analyses refer to rats of group
3 only. All values are expressed as mean ± standard deviation. For comparison of
obstructed vs. unobstructed kidneys, two-tailed paired Student t or Mann-Whitney Utest was used. For comparison of longitudinal measurements general linear model
repeated measurements with Bonferoni correction was used. Correlation of ADC with
histological markers of fibrosis was assessed with least-squares linear regression
analysis, where the Pearson's correlation coefficient r was determined and
significance was tested using F-statistics. For all tests, statistical significance was
defined as p<0.05.
10
RESULTS
MR Image Analysis
As expected and confirming the successful induction of hydronephrosis, compared to
baseline or the contralateral kidneys, the obstructed kidneys were significantly
enlarged by 20 - 30 % (p<0.001; Supplementary Figure 2, Figure 2). Compared to
baseline, slight but expected and significant hypertrophy of the contralateral kidneys
by 5 – 6 % (p<0.001) was observed at later time-points.
Compared to contralateral kidneys, on day 3 and day 5 before and after release of
the obstruction, obstructed kidneys exhibited significantly lower ADCall (9-17 %,
p<0.007) and ADClo (14-18 %, p<0.05) (Figure 1b and c). In contrast, after sacrifice,
obstructed kidneys had significantly higher ADCall (26 %, p=0.005) and ADClo (36%,
p=0.003) compared to the contralateral kidneys (Figure 1b and c). Compared to
contralateral kidneys, the ADChi of obstructed kidneys was not significantly changed
on both day 3 and day 5 before release of obstruction, but was significantly lower
after obstruction release (19%, p=0.005) and significantly higher after sacrifice (19%,
p=0.008, Figure 1a).
Compared to baseline, ADCall, ADClo and ADChi of the contralateral and obstructed
kidneys remained relatively stable on days 3 and 5 before release of the obstruction
(Figure 1a-c). After the release of obstruction, all three ADCs decreased significantly
in obstructed kidneys (by 20%, p<0.001; 25%, p=0.001; 15%, p=0.049) and less
prominently also in the contralateral kidneys (by 5 %, p=0.029; 6%, p=0.038; 4%,
p=0.3). Compared to baseline, post mortem ADCall, ADClo and ADChi dropped
significantly in both obstructed (by 50 %, 57%, 45%, all p<0.001) and contralateral
kidneys (by 61 %, 66%, 58%; all p<0.001; Figure 1a-c).
Compared to baseline, post mortem perfusion fractions of both obstructed and
11
contralateral kidneys were significantly reduced (by 74%, p<0.001; 82%, p=0.003).
The perfusion fraction of obstructed kidneys on day 5 before release was also
significantly reduced by 34% (p=0.008) and, compared to the contralateral kidney, by
42% (p=0.013) on day 3 (Figure 1d).
The absolute ADC values of the kidneys within all three animal groups were similar,
despite the variations in several DW MR imaging parameters (data now shown).
Furthermore, when ADCall values from all groups were determined, the results were
similar to those of group 3 (Figure 1b, Supplementary Figure 1d).
Histological Analysis
UUO was characterized by marked renal fibrosis. The obstructed kidneys were
enlarged, and had macroscopically obvious signs of hydronephrosis on 5 day of UUO
(Figure 3). Histomorphology and ultrastructural analyses showed no signs of post
mortem alterations, i.e. no autolysis was observed (Figure 3 and 4). Compared to the
corresponding contralateral unobstructed kidneys, UUO resulted in a significant
increase in all assessed hallmarks of renal fibrosis. The interstitial space was
expanded by 52% (p=0.015), the tubular lumen area was increased by 76%,
confirming the significant tubular dilation with tubular cell atrophy (Figure 3). Both
markers of fibrosis, i.e. collagen type I and fibronectin, were increased more than 3fold in the obstructed kidneys (Figure 3). The de novo expression of α-SMA as a
marker of accumulation of (myo-)fibroblasts showed more than 9-fold increase in the
obstructed kidneys (Figure 3). The significant expansion of the interstitial space by
matrix deposition, expansion of (myo-)fibroblasts and inflammatory cell infiltrates was
further confirmed by transmission electron microscopy (Figure 4a-c). Tubular cell
atrophy was evidenced by loss of mitochondria (Figure 4b-c).
Compared to patients with normal kidneys, patients with renal fibrosis exhibit similar
12
histopathological changes as rats with UUO, in particular regarding the expansion of
interstitial space by extracellular matrix, tubular atrophy and dilation (Figure 5).
Correlations of ADC and Fibrosis Parameters
Linear regression analysis of in vivo ADC of all b-values (ADCall) on day 5 either
before or after the release of obstruction showed a relatively weak but significant
correlation with extracellular matrix proteins collagen type I and fibronectin (
13
Table 2). Post mortem ADCall was strongly and significantly associated with all
assessed parameters of renal fibrosis with the exception of the marker of
myofibroblasts α–SMA. The strongest correlation was with tubular dilation (
14
Table 2). All correlations of post mortem ADCall with renal fibrosis markers were
positive whereas all correlations of in vivo ADCall with fibrosis markers were negative.
DISCUSSION
Our in vivo data are consistent with data from animals with renal fibrosis or patients
with CKD who all, compared to healthy kidneys, have reduced ADC in fibrotic kidneys
(13, 15, 21). The major and novel finding of this study is that, post mortem fibrotic
renal tissue permits higher random water movement compared to healthy kidneys
and thereby actually exhibits a higher rather than lower ADC.
ADC is a measure of the random Brownian motion of water molecules, which is
restricted in tissue, in particular at cellular membranes and in the cytoplasm and
organelles of cells. Accordingly, reduced ADC in tissue has been attributed to
increased cellular density in tumors and recently also to increased cellular density in
renal fibrosis (10, 22). Intuitively, this could explain the reduced ADC in renal fibrosis.
The vast majority of normal renal cortex is composed of highly organized and
differentiated columnar tubular cells with only minimal tubular lumen and
inconspicuous interstitium (23). In fibrosis, tubular cells undergo profound atrophy in
which they get flattened and lose their subcellular organelles and are eventually lost.
This is accompanied by dilation of the tubular lumen and expansion of interstitial
space. The overall number of cells is increased per area mostly due to inflammatory
infiltrates and multiplication of interstitial myofibroblasts (23). However, our detailed
histomorphological and ultrastructural analyses show that the overall area occupied
by cells despite increased cellularity is in fact significantly reduced in fibrosis. In line
with this, the tightest correlations were found between post mortem ADC and
measures of tubular dilation and interstitial expansion. In contrast, the widely
15
established parameter for analyzing the expansion of renal myofibroblasts (α-SMA),
reflecting a considerable part of the increased interstitial cellularity in fibrosis, failed to
reach significance in the correlation analyses. Hence, fibrotic renal tissue is
characterized by an increase in the area that allows random water movement and
consequently an increased ADC as we found post mortem. Despite the radical
morphological differences in kidney and liver morphology and water content, it is
noteworthy that our data are well in line with findings in experimental liver fibrosis,
showing that fibrotic livers had decreased ADC in vivo but increased ADC ex vivo
(24).
DW MR signal is no strictly mono-exponential function of the b-value, which gave rise
to the introduction of the bi-exponential intravoxel incoherent motion (IVIM) model
(25). The steeper DW signal decay observed at low b-values (< 200 s/mm2) is
attributed to non-random water motion like perfusion. Such contributions are
considered negligible at high b-values (> 400 s/mm2) that were suggested to obtain
true diffusion measurements (26). Using different combinations of four b-values up to
800s/mm², we observed a considerable drop of post mortem ADC, as compared to
baseline. The drop was highest for ADC calculated for low b-values (ADClo), which is
mainly influenced by renal function and perfusion. The post mortem perfusion fraction
was less than a quarter of the baseline value. This reduction in ADC and perfusion
fraction most likely represents the cessation of renal perfusion and function after
sacrifice (24), since kidneys exhibit higher ADC than other abdominal organs due to
the high blood supply and tubular flow and water handling (26). It could be
hypothesized that the “true” random water movement measured using our settings in
vivo represents “only” 33 - 50 % of the ADC and that fibrosis associated changes in
ADC in vivo are masked by renal function. This is also supported by the fact, that the
perfusion fraction in vivo was markedly lower in the obstructed kidneys compared to
16
the contralateral kidneys.
ADC dropped after surgical release of the obstruction comparably in both obstructed
and unobstructed kidneys. This was likely a systemic effect that resulted in altered
renal perfusion since the surgical procedure was associated with some minimal loss
of blood. Five hours after release of obstruction, the ADC returned to values
measured before the release, which suggested that the animals recovered from the
procedure. Supporting this is the finding that renal ADC sensitively reflects renal
perfusion in patients and models of renal artery stenosis, which have reduced renal
perfusion and consequently reduced ADC (13, 21, 27, 28).
The histological appearance in most, if not all, patients with renal fibrosis is
comparable to that observed in animal models. It is therefore likely that in patients,
renal fibrotic tissue also permits increased random water movement, and should be
associated with increased ADC. As in our rat model, the “real” random water
movement in humans might also be “masked” by the renal function, i.e. high bloodperfusion, filtration and water movement along the nephron. The reduced ADC in
patients with chronic kidney diseases, likely represents secondary changes
associated with fibrosis, either being reduced perfusion or reduced renal function
(directed water transport), but not fibrosis per se.
Most experimental pre-clinical studies use renal fibrosis as a major end-point in
testing new therapeutic approaches. In translational clinical studies for these targets
a fibrosis specific end-point would be most ideal. Our data suggest that DW MR
imaging might not be such a specific end-point. Furthermore, renal ADC seems to
react sensitively to both alterations of renal perfusion and water handling, e.g. after
furosemide (21, 28-30).
One of the study limitations is the relatively small sample size. However, the sample
size for the third experiment was calculated based on variability obtained from the
17
first two experiments and the results were significant. Despite the variations in DW
MR imaging parameters in the three groups, the renal ADCs were surprisingly similar
in terms of absolute values, longitudinal changes and relation of obstructed and
contralateral kidneys. Another limitation is that our model of renal fibrosis is unilateral
so that renal function remains normal and correlation analyses of renal function with
ADC are not possible.
In conclusion, our study provides insight into DW MR imaging measurement in
experimental renal fibrosis. Although our data suggest that DW MR imaging and ADC
are not specific measures of fibrosis of kidneys, its application for measurement of
associated secondary changes in renal perfusion and water handling might help us to
monitor and to learn more about renal scaring in experimental models and patients
with chronic kidney disease.
18
Acknowledgements
19
REFERENCES
1.
Boor P, Ostendorf T, Floege J. Renal fibrosis: novel insights into mechanisms and
therapeutic targets. Nat Rev Nephrol. 2010;6(11):643-56.
2.
Boor P, Sebekova K, Ostendorf T, Floege J. Treatment targets in renal fibrosis.
Nephrol Dial Transplant. 2007;22(12):3391-407.
3.
Boor P, Floege J. The renal (myo-)fibroblast: a heterogeneous group of cells. Nephrol
Dial Transplant. 2012;27(8):3027-36.
4.
Thoeny HC, De Keyzer F. Diffusion-weighted MR imaging of native and transplanted
kidneys. Radiology. 2011;259(1):25-38.
5.
Eisenberger U, Thoeny HC, Binser T, et al. Evaluation of renal allograft function early
after transplantation with diffusion-weighted MR imaging. Eur Radiol. 2010;20(6):1374-83.
6.
Thoeny HC, Binser T, Roth B, Kessler TM, Vermathen P. Noninvasive assessment of
acute ureteral obstruction with diffusion-weighted MR imaging: a prospective study.
Radiology. 2009;252(3):721-8.
7.
Thoeny HC, De Keyzer F, Oyen RH, Peeters RR. Diffusion-weighted MR imaging of
kidneys in healthy volunteers and patients with parenchymal diseases: initial experience.
Radiology. 2005;235(3):911-7.
8.
Thoeny HC, Zumstein D, Simon-Zoula S, et al. Functional evaluation of transplanted
kidneys with diffusion-weighted and BOLD MR imaging: initial experience. Radiology.
2006;241(3):812-21.
9.
Vermathen P, Binser T, Boesch C, Eisenberger U, Thoeny HC. Three-year follow-up
of human transplanted kidneys by diffusion-weighted MRI and blood oxygenation leveldependent imaging. J Magn Reson Imaging. 2012;35(5):1133-8.
10.
Togao O, Doi S, Kuro-o M, Masaki T, Yorioka N, Takahashi M. Assessment of renal
fibrosis with diffusion-weighted MR imaging: study with murine model of unilateral ureteral
obstruction. Radiology. 2010;255(3):772-80.
11.
Yang D, Ye Q, Williams DS, Hitchens TK, Ho C. Normal and transplanted rat
kidneys: diffusion MR imaging at 7 T. Radiology. 2004;231(3):702-9.
12.
Carbone SF, Gaggioli E, Ricci V, Mazzei F, Mazzei MA, Volterrani L. Diffusionweighted magnetic resonance imaging in the evaluation of renal function: a preliminary study.
Radiol Med. 2007;112(8):1201-10.
13.
Namimoto T, Yamashita Y, Mitsuzaki K, Nakayama Y, Tang Y, Takahashi M.
Measurement of the apparent diffusion coefficient in diffuse renal disease by diffusionweighted echo-planar MR imaging. J Magn Reson Imaging. 1999;9(6):832-7.
14.
Inoue T, Kozawa E, Okada H, et al. Noninvasive evaluation of kidney hypoxia and
fibrosis using magnetic resonance imaging. J Am Soc Nephrol. 2011;22(8):1429-34.
15.
Xu X, Fang W, Ling H, Chai W, Chen K. Diffusion-weighted MR imaging of kidneys
in patients with chronic kidney disease: initial study. Eur Radiol. 2010;20(4):978-83.
16.
Boor P, Celec P, Martin IV, et al. The peroxisome proliferator-activated receptor-alpha
agonist, BAY PP1, attenuates renal fibrosis in rats. Kidney Int. 2011;80(11):1182-97.
17.
Patel J, Sigmund EE, Rusinek H, Oei M, Babb JS, Taouli B. Diagnosis of cirrhosis
with intravoxel incoherent motion diffusion MRI and dynamic contrast-enhanced MRI alone
and in combination: preliminary experience. J Magn Reson Imaging. 2010;31(3):589-600.
18.
Le Bihan D, Breton E, Lallemand D, Aubin ML, Vignaud J, Laval-Jeantet M.
Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging.
Radiology. 1988;168(2):497-505.
20
19.
Boor P, Konieczny A, Villa L, et al. PDGF-D inhibition by CR002 ameliorates
tubulointerstitial fibrosis following experimental glomerulonephritis. Nephrol Dial
Transplant. 2007;22(5):1323-31.
20.
Smeets B, Boor P, Dijkman H, et al. Proximal tubular cells contain a phenotypically
distinct, scattered cell population involved in tubular regeneration. J Pathol. 2013;229(5):64559.
21.
Muller MF, Prasad PV, Bimmler D, Kaiser A, Edelman RR. Functional imaging of the
kidney by means of measurement of the apparent diffusion coefficient. Radiology.
1994;193(3):711-5.
22.
Padhani AR, Liu G, Koh DM, et al. Diffusion-weighted magnetic resonance imaging
as a cancer biomarker: consensus and recommendations. Neoplasia. 2009;11(2):102-25.
23.
Jennette JC, Olson JL, Silva FG, D'Agati V. Heptinstall's Pathology of the Kidney. 7th
edition ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2014.
24.
Annet L, Peeters F, Abarca-Quinones J, Leclercq I, Moulin P, Van Beers BE.
Assessment of diffusion-weighted MR imaging in liver fibrosis. J Magn Reson Imaging.
2007;25(1):122-8.
25.
Le Bihan D, Breton E, Lallemand D, Grenier P, Cabanis E, Laval-Jeantet M. MR
imaging of intravoxel incoherent motions: application to diffusion and perfusion in neurologic
disorders. Radiology. 1986;161(2):401-7.
26.
Notohamiprodjo M, Reiser MF, Sourbron SP. Diffusion and perfusion of the kidney.
Eur J Radiol. 2010;76(3):337-47.
27.
Yildirim E, Kirbas I, Teksam M, Karadeli E, Gullu H, Ozer I. Diffusion-weighted MR
imaging of kidneys in renal artery stenosis. Eur J Radiol. 2008;65(1):148-53.
28.
Heusch P, Wittsack HJ, Kropil P, et al. Impact of blood flow on diffusion coefficients
of the human kidney: a time-resolved ECG-triggered diffusion-tensor imaging (DTI) study at
3T. J Magn Reson Imaging. 2013;37(1):233-6.
29.
Sigmund EE, Vivier PH, Sui D, et al. Intravoxel incoherent motion and diffusiontensor imaging in renal tissue under hydration and furosemide flow challenges. Radiology.
2012;263(3):758-69.
30.
Pedersen M, Vajda Z, Stodkilde-Jorgensen H, Nielsen S, Frokiaer J. Furosemide
increases water content in renal tissue. Am J Physiol Renal Physiol. 2007;292(5):F1645-51.
TABLES
21
Table 1
MR Imaging Parameters for Group 3 (8-channel WRIST coil)
MR
Sequence
Echo /
Repetition
Time (ms)
Echo Train
Length /
EPI factor
T2w TSE
coronal
98 / 9123
61
T2w TSE
transversal
79 / 3548
DW EPI
43 / 2281
Acquisition
Resolution
(mm2)
Matrix
Section
Thickness
(mm)
Number
of
Sections
Number
of Signals
Averaged
0.45 x 0.45
256 x 150
2
17
32
43
0.45 x 0.45
156 x 108
2
16
32
49
0.80 x 0.81
64 x 136
2
16
8
22
Table 2
Linear regression analysis of ADCall and histological fibrosis markers
ADC
day 5
Fibrosis Maker
r
day 5
after release
p
r
p
day 5
after sacrifice
r
p
Tubular lumen
area
-0.211 0.510
-0.386 0.215
0.904 <0.001
Interstitial
expansion
-0.392 0.207
-0.265 0.406
0.690
0.013
Fibronectin
-0.561 0.072
-0.653 0.029
0.799
0.003
Collagen type I
-0.686 0.014
-0.643 0.024
0.727
0.007
α-SMA
-0.549 0.064
-0.504 0.094
0.558
0.059
23
Supplementary Table 1
MR Imaging Parameters for Group 1 and 2 (2-channel Flex M coil)
MR
Sequence
Group
(time
point)
T2w TSE
coronal
1 (day 3,
baseline)
83 / 3667
14
0.40 x 0.41
400 x
168/167
2.5
19
4
T2w TSE
coronal
1 (day 5),
83 / 3007
2 (all)
13
0.40 x 0.41
400 x
169
2.5
19
4
83 / 3000
14
0.40 x 0.42
120 x
167/241
2.5
16
4
T2w TSE 1 (day 5),
80 / 3511
transversal
2 (all)
17
0.40 x 0.42
176 x
114
2.5
16
4
DW EPI
1
75 / 2084
(baseline)
121
0.60 x 0.60 80 x 233
2.5
16
4
DW EPI
1 (day 3)
54 / 1340
47
0.80 x 0.81
64 x 86
2.5
16
12
DW EPI
1 (day 5),
59 / 1436
2 (all)
73
0.80 x 0.81 64 x 138
2.5
16
8
T2w TSE 1 (day 3,
transversal baseline)
Echo /
ETL /
Repetition EPI
Time (ms) factor
Acquisition
Resolution
(mm2)
Matrix
Section Number Number
Thickness
of
of Signals
(mm)
Sections Averaged
24
FIGURE LEGENDS
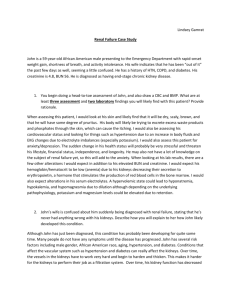
Figure 1
Longitudinal ADC and perfusion fraction in fibrotic and non-fibrotic kidneys
Longitudinal mean ADC values in the renal cortex of the obstructed (UUO) and the
contralateral kidneys from baseline (day -5) to day 5 after sacrifice computed for high
2
b-values in (a) (300, 800 s/mm : ADChi ), for all b-values in (b) (ADCall) and for low b2
values in (c) (0, 50, 300 s/mm : ADClo) and corresponding longitudinal mean
perfusion fraction in (d).
ADChi was significantly lower in obstructed (UUO) kidneys compared to contralateral
kidneys on day 5 after release of the obstruction, whereas no differences where
observed on the other time points of the in vivo measurements. Post mortem, fibrotic
kidneys had significantly higher ADChi compared to non-fibrotic kidneys. Compared to
ADChi, ADCall was more affected by renal function and perfusion. In vivo, the absolute
values were higher than ADChi (a,b). Compared to non-fibrotic kidneys, ADCall was
significantly lower in UUO on day 3 and 5 in vivo and significantly higher post
mortem (b). ADClo was mostly influenced by renal function and perfusion. Compared
to ADCall, the absolute ADC values were higher in ADClo (b, c). Similarly to ADCall the
fibrotic kidneys had reduced ADClo in vivo and increased post mortem (c). The
perfusion fraction was considerably reduced in UUO compared to contralateral
kidneys on day 3 and day 5 before obstruction release, however, significance was
only reached on day 3 (d). No difference was found on day 5 after obstruction
release. Consistently, post mortem fibrotic kidneys had significantly higher values
compared to non-fibrotic kidneys.
All data are mean ± SD, p < 0.05 (*) and p < 0.01(**).
25
Figure 2
Representative MR images
Typical coronal and transversal T2w images on day 5 before release of obstruction
(a, b) and representative ADC maps at day 3, day 5 before and after release of
obstruction and after sacrifice (c-f)
On day 5 before release, T2w images demonstrated atrophy of the UUO kidney,
enlarged ureter and renal pelvis (hydronephrosis); the renal cortex appeared
hyperintense (a, b). Development of hydronephrosis can be observed already on day
3 in the ADC map (c) and as it progressed to day 5 (d). The amount of retained urine
was reduced after release of the obstruction (e). In contrast to renal ADC in vivo, the
renal ADC after sacrifice was markedly reduced (f).
Figure 3
Histological and immunohistochemical analyses and quantification of the
obstructed and contralateral kidneys
The macroscopic appearance of the kidneys showed enlarged obstructed (left)
kidneys with initial signs of hydronephrosis (arrow) and paler color (a). Histologically,
the contralateral (CL) kidney shows a normal appearance (b,c). In obstructed kidneys
(UUO) alteration of the normal renal cortical architecture is obvious in the overview
(d). These changes encompass tubular dilation, expansion of interstitial space (d-g),
deposition of extracellular matrix (h,i, k-o), and interstitial hypercellularity composed
of (myo-)fibroblasts (j, m, p) and inflammatory infiltrates (arrowhead in e). The
quantification of tubular dilation is shown in (f) and of interstitial expansion in (g). The
analysis of tubular dilation is shown exemplary in one tubule in (c and e) in which the
tubular lumen is outlined by a region-of-interest (roi). The black area represents the
26
tubular lumen area and thereby is a measure of tubular dilation. The analysis of
interstitial expansion is shown exemplary in (c and e) by double arrows which mark
the distance between two adjacent tubular basement membranes. Compared to
normal unobstructed kidneys, the interstitial capillaries have an enlarged appearance
in UUO kidneys (asterisk in c and e). Quantification of immunohistochemistry
confirmed the more than 3-fold increase in deposition of extracellular matrix
components collagen type 1 (h, k, n) and fibronectin (i, l, o) as well as the expansion
of (myo-)fibroblasts using the α-smooth muscle actin (α-SMA) staining (j, m, p). In
unobstructed kidneys α-SMA is only expressed by vascular smooth muscle cells of
arteries and arterioles (arrow in m) but not in the interstitial space, where most of the
staining is found in UUO kidneys.
Data are mean % value ± SD, contralateral kidney was set as 100%. * p < 0.001 vs.
contralateral; n=6 per group. Periodic acid Schiff (PAS) staining (a-d), magnification
all x400 except a) and c) x100.
Figure 4
Ultrastructural changes in obstructed kidneys of rats
Contralateral kidneys show a normal ultrastructure on transmission electron
microscopy (a). Proximal tubules (PT) and distal tubules (DT) show a differentiated
phenotype with abundant mitochondria (§). The interstitial space, i.e. the space
between two tubular basal membranes, is thin (exemplary outlined by white lines).
Capillaries with erythrocytes (*) can be observed. In the obstructed kidneys (b and c),
the interstitial space is widened (white lines) by deposition of extracellular matrix
(star), expansion of (myo-)fibroblasts (Fib) and inflammatory cells (arrowhead). The
capillaries seem widened (*). The tubular cells show signs of atrophy, e.g. a
27
significant loss of mitochondria can be observed (§). Original magnification x2800.
Figure 5
Histological appearance of renal fibrosis in patients
(a) and (b) shows normal histomorphology of renal cortex from a nephrectomy due to
polytrauma in a healthy patient. In (c) and (d), a typical histology as found in patients
with advanced renal disease/fibrosis is shown. Note the dilated tubuli with flattened
(atrophied) tubular cells (arrowhead) and extensive deposition of ECM (asterisk)
leading to expansion of interstitial space (black line). In between remnants of tubular
basement membranes are found (arrows), showing the last stage of tubular loss.
These findings resemble closely those found in rats with UUO (see Figure 3).
Periodic acid Schiff (PAS) staining (a-d), magnification (a, c) all x50; (b, d) x200.
28
Supplementary Figure 1
DW image quality and longitudinal ADC for groups 1-3
DW image quality (a-c) and longitudinal ADCall (d) for groups 1-3. DW images for bvalues 50 s/mm² and 800s/mm² were rendered with the same gray level range to
illustrate DW signal decay.
DW images and ADC map acquired with the protocol of group 3 (8-channel coil, 0.8
mm in-plane resolution) on day 5 before release of obstruction is depicted in (a). DW
images and ADC map of group 2 protocol (2-channel coil, 0.8 mm in-plane resolution)
show higher noise, lower DW signal and more pronounced susceptibility effects, e.g.
at the medial and lateral surfaces of the colon, as compared to group 3 images (a, b).
Muscular ADC in group 2 appears strongly hypointense as compared to contralateral
kidney, which is not the case in group 3. This suggests insufficient signal magnitude
for b-value 800 in muscle (a, b) The same rat and anatomy as in (b) was acquired
with group 1 baseline DW sequence (2-channel coil, 0.6 mm in-plane resolution) for
the purpose of image quality comparison (c). Higher EPI factor and in-plane
resolution led to considerable susceptibility artefacts (c, arrow heads). ADC contrast
between contralateral kidney and muscle appears increased
(c, star). Despite
variation in DW sequence parameters, ADC of kidney was very similar in all groups
regarding both magnitude and difference between obstructed and unobstructed
kidney. Hence, the pooled data reinforce the findings in group 3 (Figure 1), in
particular the reversal of the ADC difference between UUO and contralateral kidney
after sacrifice.
Supplementary Figure 2
Pole-to-pole length of kidneys.
29
Differences
between
UUO
and
contralateral
kidneys
in
all
but
baseline
measurements were significant as was the enlargement of both kidneys on day 3 and
day 5 compared to baseline.
Data is mean ± SD, p<0.01 (*)