Intentional rounding with general
therapeutic observations
Michele Streatfield
Lead Nurse, OPMHN & Specialist Services
What is intentional
rounding?
It has also been called ‘comfort rounds’ or ‘care rounds’.
It is where nurses ensure that the patient’s needs are met by
observing and talking to them and asking if there is anything else
they can do for the patient before moving away from them.
It has been heavily promoted by David Cameron and the Nursing
and Care Quality Forum from 2012, and is being implemented in
nearly all hospitals.
However……
or
Cons
This can be perceived as another top down exercise not relevant for
mental health settings
Not enough research in this area
Focuses more on general hospital settings i.e. call bells, non ambulant
patients
Rounding is based in part on a study of 14 hospitals in the United States, it
may not be applicable to UK hospitals because staffing levels here tend to
be lower
Pros
Enables staff to focus general observations in a more structured way
Not just a ‘head count’
A DoH spokesperson said rounding has reduced the number of patient
complaints and significantly improved patient satisfaction levels
Looks at the service user as a whole person
Encourages interaction
Promotes positive engagement and is more therapeutic
General observations
General observation is the minimum acceptable level of
observation for all in-patients.
The primary aim of observation should be to engage
positively with the service user. This involves a two-way
relationship, established between a service user and a
staff member, which is meaningful, grounded in trust,
and therapeutic for the service user.
Nice (2005)
General observations meets
intentional rounding
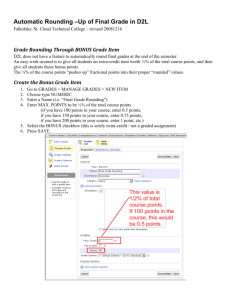
Implementation in practice
Within the 1 hour time period, staff should introduce themselves and are
advised to use the acronym ‘DONE’ as a prompt to positively engage with
and assess each patient, which stands for:
• Distress –
How is the patient feeling? How is their mental
state? Are there changes to risk?
• Observations –
How responsive are they? Are they socially isolating
themselves?
• Need –
Are they hungry or thirsty? Are they comfortable? If
relevant - Do they need assistance with toileting or
repositioning if impaired mobility? Do they need a
little reassurance?
• Environment -
Do they feel safe? Are there environmental risks?
Do they want to leave?
Adapted from Aneurin Bevan Health Board (2012)
And finally…..
The use of forms to capture this vital information
An updated form was produced by some Ward Managers and
their teams
Discussed at the Modern Matron’s Forum
Reviewing the policy using the PDSA cycle
References
•
Snelling P (2013) Intentional rounding: a critique of the evidence. Nursing Times; 109:
20, 19-21
•
National Institute for Clinical Excellence (NICE) (2005) “Violence: The short-term
management of disturbed/violent behaviour in in-patient psychiatric settings and
emergency departments”. London
•
Aneurin Bevan Health Board Newsletter (2012)
•
Kent and Medway NHS & Social Care Partnership Trust (2013) Therapeutic
observation of patients policy
 0
0