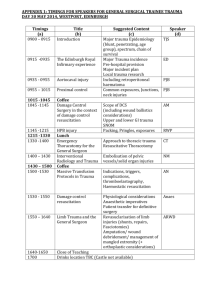
AACN Advanced Critical Care Volume 32, Number 1, pp. 64-75 © 2021 AACN Critical Care Considerations for Damage Control in a Trauma Patient Shannon Gaasch, MS, RN, CRNP-BC ABSTRACT Traumatic injury remains the leading cause of death among individuals younger than age 45 years. Hemorrhage is the primary preventable cause of death in trauma patients. Management of hemorrhage focuses on rapidly controlling bleeding and addressing the lethal triad of hypothermia, acidosis, and coagulopathy. The principles of damage control surgery are rapid control of hemorrhage, temporary control of contamination, resuscitation in the intensive care unit to restore normal physiology, and a planned, delayed definitive operative procedure. Damage control resuscitation focuses on 3 key components: fluid restriction, permissive T raumatic injury is a leading cause of death worldwide among individuals younger than 45 years and is the primary source of productive years of life lost.1 Survivors experience considerable morbidity and long-term disability, which lead to substantial increases in direct and indirect health care costs.1 Traumatic brain injury (TBI) is the single greatest cause of death after trauma, and hemorrhage is the leading cause of preventable death from trauma, with a fatality rate of 30% to 40%.1-3 In 1993 Rotondo et al4 first described early damage control strategies, which focused on the management of surgical bleeding from wounds that can be sutured, ligated, or cauterized3-5: “planned temporary sacrifice of normal anatomy to preserve vital physiology.”3 Shifting the focus from definitive treatment to rapid control of bleeding and peritoneal contamination, combined with packing the peritoneal cavity to temporize the injury and restore 64 hypotension, and fixed-ratio transfusion. Rapid recognition and control of hemorrhage and implementation of resuscitation strategies to control damage have significantly improved mortality and morbidity rates. In addition to describing the basic principles of damage control surgery and damage control resuscitation, this article explains specific management considerations for and potential complications in patients undergoing damage control interventions in an intensive care unit. Key words: damage control, permissive hypotension, resuscitation, trauma-induced coagulopathy homeostasis, revolutionized trauma care and led to a drastic reduction in mortality from hemorrhagic shock.6 This article describes the basis for damage control surgery (DCS) and damage control resuscitation (DCR), as well as the management of patients receiving care in the intensive care unit (ICU) after resuscitation. Traumatic Injury and Physiological Impact Numerous complex physiological derangements can occur after traumatic injury. Direct tissue injury generates a local response, Shannon Gaasch is Senior Nurse Practitioner II, R Adams Cowley Shock Trauma Center, University of Maryland Medical Center, 22 S Greene St, Baltimore, MD 21201 (Shannon. gaasch@umm.edu). The author declares no conflicts of interest. DOI: https://doi.org/10.4037/aacnacc2021817 VO L U M E 32 • N U MB E R 1 • S PRING 2021 Historically, coagulopathy in traumatic injury was thought to be related to fluid administration and hypothermia. Current studies, however, suggest that 30% of trauma patients present with “trauma-induced coagulopathy” (TIC)1 (Figure 2). This state develops quickly, usually within 30 minutes of injury and before significant dilution.14 Injury prompts the activation of the clotting cascade, which responds lat ion oa gu De cre as ed c sis do Coagulopathy aci Hypothermia, defined as a core body temperature less than 35 °C, can occur from physical exposure (both at the scene of injury and at the hospital), intoxication, circulatory changes, and administration of cold fluids.10 This condition is exacerbated by the loss of thermoregulatory control as a result of the uncoupling of normal metabolic pathways.10 Hypothermia has a profound impact on coagulation, inhibiting platelet aggregation and reducing coagulation factor activity by approximately 10% for every degree decrease in temperature.10,11 The severity of hypothermia has been linked with poor prognosis and may be an independent predictor of mortality in trauma: mortality rates as high as 70% to 100% have been reported in patients with severe hypothermia.1,10,12 When a trauma patient is admitted, providers should take steps to prevent hypothermia—minimizing exposure, applying warm sheets and convection blankets, administering warmed fluids, and reducing time spent in the operating room—with all efforts targeted toward achieving a core temperature higher than 35 °C.1,3,11,13 Rapid control of hemorrhage is of paramount importance in correcting hypothermia. Hypothermia c cti Hypothermia Coagulopathy La propagating a systemic reaction that can be significantly amplified and harmful.7 Rapid recognition and control of hemorrhage is critical to preventing systemic effects that may occur. In a landmark 1982 study, Kashuk et al8 first described the lethal triad of trauma (LTOT) (Figure 1), which includes hypothermia, coagulopathy, and acidosis.5 Kashuk et al observed that 89% of trauma-related deaths were attributed to hemorrhage; 51% of those patients who died had exsanguinated after satisfactory repair of vascular injury.6,8 If the characteristics of LTOT are not corrected quickly, it becomes a vicious, self-perpetuating cycle that can rapidly lead to death.1,10 CONSID E RAT IONS IN DA M AGE CONT ROL Metabolic acidosis Decreased myocardial performance Figure 1: The lethal triad in trauma. Reprinted via open access from Leibner et al.9 by forming a clot that in turn depletes platelets and coagulation factors, causing a consumptive coagulopathy. This coagulopathy is worsened by administration of crystalloid solutions and packed red blood cells (PRBCs) without the administration of clotting factors.1 Delaying transfusion of clotting products until after large quantities of PRBCs (> 10 U within 24 hours) and crystalloid have been given exacerbates coagulopathy by diluting the blood and reducing the concentration of clotting factors, further driving the cycle of the LTOT.10 Trauma-induced coagulopathy is associated with poor outcomes related to the release of inflammatory mediators from direct tissue injury and from secondary tissue hypoperfusion or cellular hypoxia, leading to systemic anticoagulation via activated protein C and depletion of clotting factors.1,3,7,10 The early development of coagulopathy after trauma is another independent predictor of mortality.14 Fibrinolysis, a key feature of TIC, occurs within the first hour after trauma and is associated with mortality rates as high as 90%.3 It is important to understand and recognize TIC early during the resuscitation phase in order to improve mortality rates; however, published clinical scoring systems designed to detect TIC do not reliably identify patients who are at risk for this complication.3 Acidosis The decreased circulatory volume derived from hemorrhage affects oxygen delivery to tissues, leading to the development of toxic metabolites, anaerobic metabolism, and lactic acidosis.10 Disruptions to pH homeostasis 65 G A ASC H W W W .AACN ACCON LIN E .ORG Preexisting conditions Age Genetics Comorbidities Preinjury medication Trauma Tissue damage Hemorrhage Shock Hypoperfusion Sympathoadrenal activation Inflammation Systemic endotheliopathy Glycocalyx shedding Endogenous heparinization Platelet activation and dysfunction Reduced clotting factor activity Hyperfibrinolysis Trauma-associated factors Resuscitation-associated factors Coagulation factor loss Coagulation factor dilution Coagulation factor consumption Hypothermia Acidosis Traumatic coagulopathy Figure 2: Trauma-induced coagulopathy. Reprinted via open access from Spahn et al.11 negatively impact enzymatic function throughout the body, and multiple organ dysfunction develops, evidenced by reduced cardiac contractility and cardiac output, vasodilatation, hypotension, and bradycardia.1,10 The degree of acidosis and the level of lactate at admission have been used to predict mortality in trauma patients.10,13 The goal is to optimize oxygen delivery through blood transfusion and augment cardiac output with pharmacologic agents while controlling hemorrhage in order to deter acidosis.10,11,15 Damage Control Surgery Rotondo et al4 described DCS in the management of penetrating abdominal injuries 66 and enumerated 3 distinct phases: (1) surgical control of hemorrhage and contamination followed by intraperitoneal packing and temporary closure of the abdomen; (2) resuscitation of the patient in the ICU in order to reverse coagulopathy and achieve normal physiology; and (3) definitive surgical management once normal physiology has been restored.4,5,10,15 This strategy significantly reduced mortality from 89% to 23%, and it can also be applied in patients with musculoskeletal trauma, in whom temporary stabilization with external fixation can reduce hemorrhage and mortality.10,16 The initial goal is to correct metabolic derangements and restore normal physiology, rather than provide definitive VO L U M E 32 • N U MB E R 1 • S PRING 2021 CONSID E RAT IONS IN DA M AGE CONT ROL Table 1: Indications for Damage Control Resuscitationa Anatomic Parameters Estimated ISS > 36 Penetrating abdominal injuries Penetrating chest injuries Open pelvic fracture Long bone fracture with head injury Long bone fracture with lung contusion Truncal hemorrhage and amputation Physiologic Parameters Weak or absent radial pulse Core body temperature < 35 °C Systolic BP < 100 mm Hg Heart rate > 100 PaO2/FiO2 < 250 Urinary output < 50 mL/h Lab Parameters Lactate > 2.5 mmol/L Platelet count < 90 000/mL Fibrinogen > 1 g/dL PT > 16 s INR > 1.5 Hg < 11 pH < 7.2 Base deficit < 6 Abbreviations: BP, blood pressure; FiO2, fraction of inspired oxygen; Hg, hemoglobin; INR, international normalized ratio; ISS, injury severity score; PaO2, partial pressure of oxygen; PT, prothrombin time. a Reprinted via open access from Giannoudi and Harwood.10 surgical control, particularly for patients who display evidence of imminent demise.5 In phase 1, the goal of surgery is to achieve hemostasis through direct or indirect measures (eg, packing, aortic balloon occlusion, stabilization of fractures) and to control peritoneal contamination.11,15,17 Once this goal is achieved, the surgeon packs the abdomen, applying direct pressure to tamponade bleeding from solid organs, then temporarily closes the wound with simple skin closure or by applying a vacuumsealing device.11,15,17 Ideally, this phase should be performed within 90 minutes to decrease significant metabolic derangements. The patient is then transferred to the ICU, where resuscitation and reversal of metabolic derangements can be continued. The goal is to reverse coagulopathy and hypothermia, and restore a normal acid-base status. When the patient becomes stable they are taken back to the operating room where the surgeon attempts definitive treatment; ideally, this occurs within 24 hours of DCS surgery.17 Damage Control Resuscitation During the past decade, a new concept of DCR has emerged as a result of improved understanding of the negative impact the LTOT has on morbidity and mortality. Often used in combination with DCS,5 DCR was designed to support actively bleeding trauma patients by restoring homeostasis and preventing or mitigating tissue hypoxia, oxygen debt, and coagulopathy.3,18 A systematic approach to major trauma minimizes blood loss and optimizes patient outcomes, resulting in dramatically reduced mortality from hemorrhage and a lower incidence of—and less severe—complications such as multiple organ dysfunction and infection.3 The success of this approach requires a coordinated effort and multidisciplinary approach.3 Damage control resuscitation should be initiated upon the first contact with the patient in the prehospital environment and should continue throughout care until hemorrhage is controlled and physiology corrected.10 Patients who have a major abdominal or thoracic visceral injury, significant pelvic trauma, amputation, multiple longbone fractures, or head injury have a high risk for deterioration and should be evaluated as candidates for DCR3,19 (Table 1). The core principles of DCR are permissive hypotension, fluid restriction, and fixed-ratio blood product transfusion5,11 (Figure 3). Permissive Hypotension Targeting a normal blood pressure (BP) has been associated with worse outcomes in patients with active hemorrhage. The exception is patients with TBI or spinal cord injury, who require a higher perfusion pressure to preserve neural tissue.5,10 Resuscitation to a normal BP can displace clots formed during the body’s attempt to achieve primary hemostasis and will likely lead to dilutional coagulopathy as a result of overresuscitation, causing more bleeding and worsening tissue perfusion.3,5,10 The goal of permissive hypotension is to achieve the minimal BP necessary to perfuse organs. Current data suggest a target systolic BP of 80 to 100 mm Hg.9 For patients with TBI who are 50 to 69 years old, a desirable systolic BP target is more than 100 mm Hg; for such patients who are younger than 49 years, a systolic BP more than 110 mm Hg should be targeted.9,20 These values equate to restoration of a palpable radial pulse. Permissive hypotension has been linked with improved mortality in trauma patients, likely because 67 G A ASC H W W W .AACN ACCON LIN E .ORG Rapid diagnosis Limit crystalloids Antifibrinolytics Damage control resuscitation Rapid anatomic control Early 1:1:1 transfusion strategy Permissive hypotension Figure 3: Principles of damage control resuscitation. 1:1:1 transfusion strategy is 1 packed red blood cells: 1 plasma: 1 platelet. Reprinted via open access from Leibner et al.9 of fluid restriction and not the specific BP target.9,21,22 Although this strategy has been linked to improved survival rates, it should be used with caution in elderly patients and patients with chronic hypertension.21 Once bleeding has been controlled, a normal BP should be obtained.2 Fluid Restriction Aggressive fluid resuscitation in an actively hemorrhaging patient leads to increased bleeding and dilutional coagulopathy. Administration of large volumes of fluid may temporarily increase BP, but it counteracts compensatory vasoconstriction and innate primary hemostasis, leading to more hemorrhage and rebleeding from spontaneously clotted vessels.3 Advanced Trauma Life Support recommendations have changed from “aggressive resuscitation” to a more balanced approach, endorsing a maximal infusion of 1 L isotonic crystalloid solution and early transfusion of blood products.1,13,23 Further administration of fluids is then guided by an assessment of the patient’s responsiveness to the administered fluids.23 Ultimately, large volumes of intravenous fluid negatively impact organ function.3 Patients with a high crystalloid-to-PRBC ratio during the first 24 hours have increased 68 mortality and higher rates of acute respiratory distress syndrome (ARDS), multiple organ dysfunction, and abdominal compartment syndrome (ACS) than patients without a high crystalloid-to-PRBC ratio; the abdominal viscera can sequester liters of fluid and can double in size after resuscitation with massive amounts of intravenous fluids.1,5 In a retrospective study, Neal et al24 found that a crystalloid-to-PRBC ratio more than 1.5:1.0 in patients receiving massive transfusions was associated with a 70% higher risk of multiple organ failure and a 2 times higher risk of ARDS and ACS.9,24 A fluid-restrictive guideline, as suggested in the Advanced Trauma Life Support manual,23 is recommended. Balanced crystalloid solutions should preferentially be administered, whereas normal saline solutions should be avoided because of the high incidence of hyperchloremic acidosis and renal failure.11 Fixed-Ratio Blood Transfusion Historically, large-volume infusions of crystalloid solution and PRBCs were administered before plasma and platelet transfusions would be considered, contributing to dilutional coagulopathy and other complications in severely injured patients. Landmark studies from the US military demonstrated a significant survival advantage in patients who received infusions with higher ratios of fresh frozen plasma to PRBCs.5,25-28 This survival benefit, however, was not demonstrated in a large, multicenter civilian study.29 Unlike crystalloid transfusion, balanced product transfusion resolves acidosis, prevents endothelial damage, treats TIC, and begins to reverse (rather than contribute to) DC.1 Early use of platelets in a balanced transfusion strategy has been associated with improved survival after trauma.1,18 Fixed-ratio transfusions—defined as transfusion of PRBCs, plasma, and platelets at a 1:1:1 ratio—are effective in approximating the makeup of whole blood; in addition, administration of cryoprecipitate should be considered during administration of large amounts of blood products.1,5,18 The Eastern Association for the Surgery of Trauma consensus practice guidelines suggest that early resuscitation with blood product (ie, plasma and platelets) followed by administration of PRBCs is a safe guiding principle, though further data are needed to support this recommendation.25 The therapeutic targets for DCR are outlined in VO L U M E 32 • N U MB E R 1 • S PRING 2021 CONSID E RAT IONS IN DA M AGE CONT ROL Table 2: Therapeutic Goals During Damage Control Resuscitation Without Neurotrauma With Neurotrauma Arterial pressure (mm Hg) Before hemostasis: 80 < systolic BP < 100 After hemostasis: MAP > 65 Before and after hemostasis: systolic BP > 100 or MAP > 80 Hemoglobin (g/dL) 7-9 7-9 International normalized ratio <2 < 1.5 Platelet count/mm > 50 000 > 100 000 Calcium (mmol/dL) > 10 Fibrinogen (mg/dL) 150-200 pH > 7.2 Temperature (°C) > 36 3 Abbreviations: BP, blood pressure; MAP, mean arterial blood pressure. Reprinted via open access from Malgras et al.17 Table 2. Point-of-care thromboelastography may help detect coagulation abnormalities and allow for a targeted goal-directed transfusion strategy.11 Hypocalcemia is a common complication associated with blood transfusions; the citrate added to stored blood in order to prevent coagulation binds to calcium in the serum. Calcium, in its free ionized state, is present in the extracellular plasma and is essential in the formation and stabilization of fibrin, assists in platelet function, and is important for cardiac contractility and for maintaining systemic vascular resistance.11 Platelet and plasma transfusion products require even higher citrate concentrations, making hypocalcemia more likely to occur than when PRBCs alone are administered.11,13 Care Considerations in the ICU After DCS the patient is transferred to the ICU for continued resuscitation until their transition to the postresuscitation phase of care. The primary management strategies are to prevent and mitigate the LTOT by avoiding hypothermia, correcting acidosis, reversing coagulopathy, and assessing for ongoing bleeding. An initial evaluation should focus on the presence and extent of shock, hemodynamics, end-organ perfusion, intravascular volume status, neurologic examination, and a general head-to-toe survey of injuries. After initially resuscitating the patient, nurses should focus attention on common ICU considerations such as ensuring a patent airway, maintaining ventilatory status, providing sufficient nutrition, managing pain, preventing and treating delirium, promoting early mobility, and avoiding potential complications—all of which help optimize outcomes for patients who undergo DCS. End Points of Resuscitation One common misconception by clinicians in the ICU is that vital signs can be relied on to diagnose hypovolemia, whereas various clinical conditions that cause vital signs to change may not necessarily represent hypovolemia.30,31 Shock is the consequence of inadequate tissue perfusion, which results in metabolic acidosis. The presence and extent of shock are evident through altered physiologic parameters such as serum lactate and arterial blood gas (but not necessarily BP). Patients with severe shock may also have “normal” vital signs as compensatory mechanisms transiently maintain BP in the face of profound metabolic acidosis.32 This phenomenon is particularly evident in young trauma patients. Several modalities are available to assess hemodynamics and volume status, including echocardiography and invasive and noninvasive hemodynamic monitoring; each has advantages and disadvantages.33,34 Static indices give a representation of the cardiac preload; they do not, however, accurately predict responsiveness to fluid administration.35 Such indices include central venous pressure, pulmonary artery occlusion pressure, and right ventricular end-diastolic volume.36 Dynamic indices allow a better understanding of a patient’s volume 69 G A ASC H status and help determine whether the patient should receive fluid or a vasopressor. The passive leg raise maneuver is a dynamic assessment that has been validated and in use for many years. If the patient will respond to fluids, a 10% to 12% increase in cardiac output and stroke volume will occur when the legs are passively raised.35 Bedside ultrasonography has become an invaluable tool in determining intravascular volume.31 The clinician should first determine fluid volume via point-of-care ultrasound, then evaluate the patient’s responsiveness to fluids. Collapse of the inferior vena cava during the respiratory cycle implies that the patient would respond to fluids. Because of the impact of changes in thoracic pressure on the inferior vena cava, irregular respiratory mechanics limit the applicability this assessment method.37 Assessing left ventricular size and function can help determine fluid status: if the patient has a small, hyperdynamic left ventricle with “kissing ventricles,” hypovolemia is likely to be present.37 After assessing fluid status and cardiac function, the clinician should determine responsiveness to fluids.31 Stroke volume variation is typically measured on the basis of the velocity time integral (VTI) through point-ofcare ultrasound in patients receiving positivepressure ventilation. The VTI measures the velocity at and distance to which blood ejects during each myocardial contraction.31,37 Clinicians should obtain multiple measurements of VTI. A VTI variation greater than 12% indicates that the patient will respond to fluids; variation more than 14% is highly predictive of fluid responsiveness, whereas variation less than 10% is a highly negative predictive value.31,37 When used together, VTI measurements and the passive leg raise test provide an ideal assessment of fluid responsiveness.35 A concern with using point-of-care ultrasound to assess intravascular volume is the variability of clinicians’ skill in performing the study.31,37 Lactate and base deficit are markers of anaerobic metabolism, and trends should be analyzed in order to track recovery from shock at the cellular level.11,30 The level of lactate, produced through anaerobic glycolysis, has prognostic value in patients with hemorrhagic shock: an elevated level in serum is associated with an increased risk of death and a likelihood of infectious complications and multiorgan failure.11 Early clearance of lactic 70 W W W .AACN ACCON LIN E .ORG acidosis correlates with improved survival.11 Base deficit, measured through arterial blood gas, is an indirect estimation of global tissue acidosis due to impaired perfusion; it more reliably identifies shock 24 hours after presentation, by which time the effects of shock have been established.11,31,38,39 The time to clear a base deficit has not been correlated with prognosis, and lactate may have better clinical applicability after resuscitation with intravenous fluids.30 Many factors can affect base deficit, including gastrointestinal losses, diabetic ketoacidosis, and renal dysfunction— again making lactate a more reliable marker.31 Lactate may, however, be less accurate than base deficit in patients with concurrent liver failure. Persistent metabolic acidosis indicates ongoing blood loss or inadequate resuscitation; sodium bicarbonate should not be administered to treat acidosis related to hypovolemic shock.23 If a nurse suspects ongoing blood loss, they should notify the surgeon, who can then assess the need for reexploration or angioembolization. Urine output can be a surrogate for adequate renal blood flow, though this has limitations. Acceptable urine output is 0.5 mL/kg/h in adults.23 Airway and Ventilation Management Airway and ventilation complications are the most common issues identified during the early management of severely injured patients.23,30 Signs of sudden or rapidly progressive desaturation—which may or may not be accompanied by tachycardia, arrhythmia, and agitation—should be evaluated as an airway emergency.30 Pulse oximetry is essential to recognizing inadequate peripheral arterial oxygenation and allows immediate assessment of interventions to improve oxygenation.23 An advanced airway (eg, endotracheal intubation, surgical airway) should be placed in patients who have altered mental status (Glasgow Coma Scale score < 8); are severely agitated or apneic; have multiple complex facial fractures, inhalation injury, neck hematoma, or a laryngeal or tracheal injury; have severe metabolic disturbances; or are unable to maintain a patent airway.23 One common sequela of traumatic injury is ARDS, which is a result of the neurohormonal and inflammatory responses that occur after injury. Patients with thoracic trauma are at particularly high risk for this complication.40 VO L U M E 32 • N U MB E R 1 • S PRING 2021 Lung-protective ventilation strategies can prevent secondary lung injury and ARDS.40 Secondary and Tertiary Survey The primary survey of the patient is completed upon their arrival in the trauma bay, addressing life-threatening injuries. A secondary survey begins after airway, breathing, and circulatory concerns have been addressed and resuscitation has been initiated.23 When the patient is transferred to the ICU, a head-totoe assessment is completed to identify other potential injuries, radiographs and laboratory tests are ordered to further investigate potential injuries, and fractures are stabilized.23 Despite this thorough assessment and initial workup, injuries are occasionally missed until a tertiary survey is performed.30 A full head-totoe examination in the ICU is imperative; the nurse should assess for tenderness and joint stability once the patient is clinically stable. Such extended assessment has reduced the number of missed injuries by 40% to 57%.30,41 Nutrition Critical illness produces a catabolic state, making nutrition exceedingly important; sometimes, however, it is overlooked. Guidelines recommend that full enteral nutrition (EN) be initiated within 24 to 48 hours of admission to the ICU to maintain gut integrity, modulate the systemic inflammatory response, and reduce mortality and infectious morbidity.36,42,43 Enteral nutrition should, however, be delayed in patients with intestinal discontinuity or high-output fistulas.44 Barriers to providing sufficient EN exist because of the multiple interruptions in therapy that often occur for surgical and procedural interventions; an estimated 60% of interruptions to enteral feeding in the ICU are due to fasting for procedures.42 A randomized controlled trial demonstrated that EN can be safely continued in intubated patients until their operation and is not associated with a higher risk of aspiration.42 Traumatic injury results in dramatic changes in metabolism and the body’s utilization of lean tissue to support gluconeogenic substrates and immune repair functions.43 The hormonal stress response overrides the normal starvation pattern that preserves lean muscle, instead promoting progressive loss of skeletal muscle.43 Survival is strongly correlated with early EN, and thus it is recommended for patients with CONSID E RAT IONS IN DA M AGE CONT ROL TBI.43 This patient population has high energy and protein requirements as a result of the significant catabolic state that accompanies TBI.43 Patients with an open abdomen have increased fluid, electrolyte, and protein requirements because of large-volume losses—an estimated 2.0 to 4.6 g of nitrogen are lost per liter of abdominal fluid output—putting them at risk of being underfed.36 Enteral nutrition may still be considered safe in patients who require vasopressors, although they should be monitored closely for signs of intolerance to enteral feeding (eg, abdominal distention, increasing gastric tube output or gastric residuals, decreased passage of flatus or stool, worsening metabolic acidosis and base deficit); if such signs are present, the patient should be evaluated for intestinal ischemia.43 Promotility agents should be initiated for patients with gastroparesis and high risk for aspiration. Although these agents improve gastric emptying and tolerance of EN, studies have not demonstrated any significant impact on clinical outcome in patients in the ICU.43 Last, glucose control is important in critically ill patients, and glucose should be maintained at 150 to 180 mg/dL.43 Tight glucose control (defined as 80 to 110 mg/dL) is associated with higher risk of hypoglycemia and mortality.43 Pain Management Multimodal analgesia is essential for all surgical patients. A patient’s pain regimen should be tailored to their individual injury and clinical situation; such customization requires multidisciplinary collaboration.45 The use of multimodal analgesia reduces opioid use and opioid-related adverse effects, and enhances the patient’s postoperative recovery, function, and satisfaction.45 Multimodal analgesia is achieved by administering nonopioid medications (eg, nonsteroidal anti-inflammatory drugs, acetaminophen, gabapentinoids, N-methyl-D-aspartate receptor antagonists, _2 agonists, or a combination of them) synergistically with opioid medications.45 Excessive use of opioids has many deleterious effects such as confusion, sedation, hypotension, constipation, and respiratory depression—to name only a few—and prolonged use of opioids can lead to physical dependence and addiction.45 Additional approaches to pain management, such as patient-controlled analgesia and neuroaxial or peripheral nerve blocks, can also be considered.45 71 G A ASC H Nonpharmacologic interventions such as massage, guided imagery, distraction, and cold compresses decrease pain, anxiety, and opioid use, and should also be incorporated.45 Delirium and Early Mobility Delirium is a common problem that affects up to 90% of hospitalized patients and is associated with longer hospital length of stay, more ventilator days, higher cost of care, and long-term cognitive impairment.46 The incidence of delirium is high among patients in the ICU: delirium affects up to 80% of mechanically ventilated patients.46 Delirium is defined as an acute change in mental status from baseline, and patients are unable to maintain or focus attention for a sustained period of time.46 Risk factors include medications, older age, multiple comorbidities, prolonged mechanical ventilation, major surgery, and septic shock.46 Nurses should use validated tools to screen for the presence of delirium; the Confusion Assessment Method for the Intensive Care Unit and Intensive Care Delirium Screening Checklist are among the most widely used tools.46 Prevention of delirium is crucial, and nurses should emphasize interventions embodied in the ABCDEF bundle: assess, prevent, and manage pain; both spontaneous awakening and spontaneous breathing trials; choice of analgesia and sedation; assess, prevent, and manage delirium; early mobility and exercise; and family engagement and empowerment.47,48 Examples of strategies aimed at preventing delirium include performing sleep hygiene, promoting normal circadian rhythms, reducing noise, frequently reorienting the patient, mobilizing early, minimizing sedation, and avoiding use of benzodiazepines.46-48 Pharmacologic treatment with typical and atypical antipsychotic drugs has not decreased the incidence of delirium and may have associated harmful effects (QT prolongation, neuroleptic malignant syndrome, and oversedation).46 Early mobility reduces ICU and hospital lengths of stay, delirium, and mechanical ventilation days and increases functional independence at discharge.49 Unfortunately, early mobility is not always feasible in trauma patients because of mobility restrictions and ongoing resuscitation needs, which may render the patient immobile for prolonged periods. Myopathy and neuropathy are complications that can develop in patients in the ICU and 72 W W W .AACN ACCON LIN E .ORG occur in one-third of critically ill patients as a result of muscle wasting; these conditions can leave patients with permanent residual mobility limitations.50 Bed rest is the most common modifiable risk factor.50 A multidisciplinary approach to early mobility is imperative to reducing the incidence of ICU-acquired weakness. Prophylaxis for Venous Thromboembolism Hospital-acquired venous thromboembolism occurs in more than 50% of patients who sustain multiple traumatic injuries; pulmonary embolism is the third leading cause of death among those who survive the first 72 hours after injury.11 Early mechanical prophylaxis is encouraged, and European guidelines recommend initiating pharmacologic prophylaxis for venous thromboembolism within the first 24 hours after bleeding has been controlled, although commencement may be delayed if concern exists about a hemorrhagic neurologic injury.11 Low-molecular-weight heparin (eg, enoxaparin) is recommended as such a prophylaxis (unless it is contraindicated).51 Complications Related to DCS and DCR Transfusion-Related Acute Lung Injury One of the risks associated with administration of blood products is the development of transfusion-related acute lung injury, a syndrome of noncardiogenic pulmonary edema associated with hypoxia.52 The diagnostic criteria include onset of symptoms within 6 hours of blood transfusion in the absence of other clinical conditions that could lead to acute lung injury.52 Patients may become tachycardic, febrile, hypotensive, and hypoxemic, and radiographs may show evidence of bilateral chest infiltrates, without signs of fluid overload.50 In such cases, blood transfusion should be terminated; low-tidal-volume ventilation may be initiated, as the pathophysiology for transfusion-related acute lung injury mimics that of ARDS.52 ACS and Intra-abdominal Ischemia Patients who develop ACS can deteriorate rapidly and develop progressive hypotension with a transient fluid response.36 If ACS goes unrecognized and untreated, it can lead to reduced pulmonary compliance and worsening respiratory acidosis, ultimately developing into metabolic acidosis as a result of hypoperfusion.36 VO L U M E 32 • N U MB E R 1 • S PRING 2021 Abdominal distention can worsen and elevated airway pressure, hypoxia, oliguria, or anuria can occur in patients with ACS; a bladder pressure more than 20 cm H2O with new organ dysfunction or failure is diagnostic of the condition.5,44,53 The risk of developing ACS is lower with DCR than with traditional resuscitation methods, despite whether temporary or definitive closure has occurred.5 If rapid decompression is required, circulatory collapse can occur from the sudden reestablishment of perfusion and the associated acid washout. High minute ventilation and administration of sodium bicarbonate and calcium can help stabilize the patient in this circumstance.36 In severe shock, circulation is preferentially shunted away from the gastrointestinal tract to the vital organs, especially if a patient requires a high-dose vasopressor.22 Mesenteric venous return can be impaired in patients with intra-abdominal packing or increased intra-abdominal pressure, and they may develop congestive intestinal ischemia.36 As intravascular volume is replete with intravenous fluid, the compromised bowel is reperfused and mucosal damage caused by free radicals may occur, followed by worsened bowel edema.36 Failure to Achieve Primary Closure Inability to close the fascia in a patient with a midline abdominal wound is the most feared complication of temporary abdominal closure and is independently associated with increased mortality.6,36 Patients in whom surgeons are able to close the abdomen during the first return to the operating room have a lower risk for pulmonary, wound, infectious, and noninfectious complications.5 Volume overload, prolonged duration of an open abdomen, and development of enterocutaneous fistulas or intra-abdominal abscesses are risk factors for the inability to achieve primary closure.36 Failure to close the fascia results in a large ventral hernia, and the patient will require abdominal wall reconstruction. These patients have a high risk for infection and enteroatmospheric fistulas.36 Vacuum-mediated closure methods are preferred for temporary skin closure following trauma-related DCS because they allow peritoneal effluent to drain while providing fascial traction toward the midline.6 Direct peritoneal resuscitation by continuously irrigating the peritoneal cavity and removing inflammatory cytokines has CONSID E RAT IONS IN DA M AGE CONT ROL been associated with fewer intra-abdominal infections, a shorter time to definitive abdominal closure, and lower mortality rates.54 Infection-Related Considerations Trauma patients are at risk for a number of infectious complications because of alterations in immune defense, disruption of tissue integrity, and the effects of indwelling catheters.44 Patient-specific risk factors (eg, age, sex, and comorbidities) and the mechanism of trauma (eg, site of injury) contribute to the risk of posttraumatic nosocomial infections.44 Prophylactic antibiotics should be administered early to patients with a penetrating abdominal or brain injury or an open fracture.30 Preoperative administration of antimicrobial prophylaxis is recommended for patients undergoing colon, neurosurgical, head and neck, cardiothoracic, vascular, facial, and orthopedic procedures.55 Patients with an open abdomen are at an increased risk of infectious complications: about one-quarter of such patients develop wound infections, deep abdominal abscesses, or intestinal fistulas.36,44 The risk of infectious complications, including bloodstream infections, increases after 8 days of having an open abdomen because of an inability to achieve primary fascial closure.36 Pneumonia is a common complication among patients in the ICU and occurs secondary to prolonged intubation and sequelae from the injury that alter mental status or pulmonary mechanics.44 Aspiration pneumonia is particularly prevalent; severely ill trauma patients with brain injury or a depressed level of consciousness are at high risk. Individuals who experience microaspiration typically require a longer ICU stay and prolonged mechanical ventilation.44 Diligence in providing measures to prevent ventilator-associated pneumonia, including elevating the head of the bed more than 30°, providing oral hygiene with chlorhexidine mouthwash, and minimizing the use of sedatives and narcotics, can reduce the incidence of the condition.43 Trauma patients and those with complicated injury patterns are at risk for urinary tract infections and bloodstream infections related to prolonged use of invasive devices during the resuscitative phase.44 When a patient requires a catheter, nurses should use proper sterile insertion technique, when feasible; catheters that were placed emergently should be replaced within 24 hours, and early removal is recommended. Clinician 73 G A ASC H collaboration with pharmacists and infectious disease specialists is encouraged in order to prevent and treat infectious complications among patients in the ICU. Conclusion Significant physiologic and metabolic derangements occur after a traumatic injury. Wartime experiences have provided a better understanding of the pathophysiology of trauma and coagulopathy and have led to revolutionary changes in management and resuscitation strategies. When used synergistically, DCS and DCR considerably improve morbidity and mortality rates. The central focus of DCR includes permissive hypotension, minimizing fluid administration, and balanced blood product transfusion; hemorrhage must also be controlled early. These approaches require multidisciplinary collaboration to recognize signs of a patient’s imminent demise or TIC so that treatment can be promptly initiated to halt the LTOT, thereby reducing hemorrhage and any resulting sequelae. REFERENCES 1. Cantle PM, Roberts DJ, Holcomb JB. Damage control resuscitation across the phases of major injury care. Curr Trauma Rep. 2017;3(3):238-248. doi:10.1007 /s40719-017-0096-9 2. Boukerrouche A. Damage control strategy. Acta Sci Gastrointest Dis. 2019;2(6):47-51. doi:10.31080/ asgis.2019.02.0065 3. Heim C, Steurer M, Brohi K. Damage control resuscitation: more than just transfusion strategies. Curr Anesthesiol Rep. 2016;6(1):72-78. doi:10.1007/s40140-016-0145-x 4. Rotondo MF, Schwab CW, McGonigal MD, et al. “Damage control”: an approach for improved survival in exsanguinating penetrating abdominal injury. J Trauma. 1993; 35(3): 375-382; discussion 382-383. doi:10.1097/00005373199309000-00008 5. Beldowicz BC. The evolution of damage control in concept and practice. Clin Colon Rectal Surg. 2018;31(1): 30-35. doi:10.1055/s-0037-1602177 6. Hu P, Uhlich R, Gleason F, Kerby J, Bosarge P. Impact of initial temporary abdominal closure in damage control surgery: a retrospective analysis. World J Emerg Surg. 2018;13:43. doi:10.1186/s13017-018-0204-3 7. Dutton RP. Resuscitative strategies to maintain homeostasis during damage control surgery. Br J Surg. 2012; 99(suppl 1):21-28. doi:10.1002/bjs.7731 8. Kashuk JL, Moore EE, Millikan JS, Moore JB. Major abdominal vascular trauma—a unified approach. J Trauma. 1982;22(8):672-679. 9. Leibner E, Andreae M, Galvagno SM, Scalea T. Damage control resuscitation. Clin Exp Emerg Med. 2020;7(1): 5-13. doi:10.15441/ceem.19.089 10. Giannoudi M, Harwood P. Damage control resuscitation: lessons learned. Eur J Trauma Emerg Surg. 2016; 42:273-282. doi:10.1007/s00068-015-0628-3 11. Spahn DR, Bouillon B, Cerny V, et al. The European guideline on management of major bleeding and coagulopathy following trauma: fifth edition. Crit Care. 2019;23(1):98. doi:10.1186/s13054-019-2347-3 74 W W W .AACN ACCON LIN E .ORG 12. Inaba K, Teixeira PG, Rhee P, et al. Mortality impact of hypothermia after cavitary explorations in trauma. World J Surg. 2009;33(4):864-869. 13. Mizobata Y. Damage control resuscitation: a practical approach for severely hemorrhagic patients and its effects on trauma surgery. J Intensive Care. 2017;5(4). doi:10.1186/s40560-016-0197-5 14. MacLeod JB, McKenney LM, Cohn SM, Murtha M. Early coagulopathy predicts mortality in trauma. J Trauma. 2003;55(1):39-44. 15. Shapiro MB, Jenkins DH, Schwab CW, Rotondo MF. Damage control: collective review. J Trauma. 2000;49(5):969-978. 16. Scalea TM. Optimal timing of fracture fixation: have we learned anything in the past 20 years? J Trauma. 2008; 65(2):253-260. 17. Malgras B, Prunet B, Lesaffre X, et al. Damage control: concept and implementation. J Visc Surg. 2017;154(suppl 1): S19-S29. doi:10.1016/j.jviscsurg.2017.08.012 18. Cap AP, Pidcoke HF, Spinella P, et al. Damage control resuscitation. Mil Med. 2018;183(suppl 2):36-43. doi:10.1093/milmed/usy112 19. Kalkwarf KJ, Cotton BA. Resuscitation for hypovolemic shock. Surg Clin North Am. 2017;97(6):1307-1321. 20. Chang R, Holcomb JB. Optimal fluid therapy for traumatic hemorrhagic shock. Crit Care Clin. 2017;33(1):15-36. doi:10.1016/j.ccc.2016.08.007 21. Kudo D, Yoshida Y, Kushimoto S. Permissive hypotension/hypotensive resuscitation and restricted/controlled resuscitation in patients with severe trauma. J Intensive Care. 2017;5(11). doi:10.1186/s40560-016-0202-z 22. Morrison CA, Carrick MM, Norman MA, et al. Hypotensive resuscitation strategy reduces transfusion requirements and severe postoperative coagulopathy in trauma patients with hemorrhagic shock: preliminary results of a randomized controlled trial. J Trauma. 2011;70(3):652-663. 23. American College of Surgeons. Advanced trauma life support (ATLS®): the tenth edition. J Trauma Acute Care Surg. 2013;74(5):1363-1366. https://viaaerearcp.files. wordpress.com/2018/02/atls-2018.pdf 24. Neal MD, Hoffman MK, Cuschieri J, et al. Crystalloid to packed red blood cell transfusion ratio in the massively transfused patient: when a little goes a long way. J Trauma Acute Care Surg. 2012;72:892-898. 25. Cannon JW, Khan MA, Raja AS, et al. Damage control resuscitation in patients with severe traumatic hemorrhage: a practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg. 2017;82:605-617. doi: 10.1097/ TA.0000000000001333 26. Holcomb JB, Pati S. Optimal trauma resuscitation with plasma as the primary resuscitative fluid: the surgeon’s perspective. Hematology Am Soc Hematol Educ Program. 2013;2013:656-659. 27. US Army Institute of Surgical Research. Joint Theater trauma system clinical practice guideline: damage control resuscitation at level IIb/III treatment facilities. Originally released December 18, 2004. Approved February 1, 2013. Accessed September 18, 2020. http://www. usaisr.amedd.army.mil/assets/cpgs/Damage%20Control%20Resuscitation%20-%201%20Feb%202013.pdf 28. Borgman MA, Spinella PC, Perkins JG, et al. The ratio of blood products transfused affects mortality in patients receiving massive transfusions at a combat support hospital. J Trauma. 2007;63(4):805-813. 29. Holcomb JB, Tilley BC, Baraniuk S, et al; PROPPR Study Group. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015;313(5):471-482. 30. Garcia A. Critical care issues in the early management of severe trauma. Surg Clin North Am. 2006;86(6):13591387. doi:10.1016/j.suc.2006.07.004 31. Kelley KC, Dammann K, Alers A, Zanders TB, Bendas C, Stawicki SP. Resuscitation endpoints in traumatic shock: VO L U M E 32 • N U MB E R 1 • S PRING 2021 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. a focused review with emphasis on point-of-care approaches [Online first]. IntechOpen. 2020. doi:10.5772/ intechopen.90686 Deane M, Galvagno SM Jr, Moran B, Stein DM, Scalea TM, O’Connor JV. Shock, not blood pressure or shock index, determines the need for thoracic damage control following penetrating trauma. Shock. 2020;54(1):4-8. Jozwiak M, Monnet X, Teboul JL. Less or more hemodynamic monitoring in critically ill patients. Curr Opin Crit Care. 2018;24(4):309-315. Jozwiak M, Monnet X, Teboul J-L. Monitoring: from cardiac output monitoring to echocardiography. Curr Opin Crit Care. 2015;21(5):395-401. Wise R, Faurie M, Malbrain MLNG, Hodgson E. Strategies for intravenous fluid resuscitation in trauma patients. World J Surg. 2017;41(5):1170-1183. doi:10.1007/s00268-016-3865-7 Chabot E, Nirula R. Open abdomen critical care management principles: resuscitation, fluid balance, nutrition, and ventilator management. Trauma Surg Acute Care Open. 2017;2(1):e000063. doi:10.1136/tsaco-2016-000063 Martin ND, Codner P, Greene W, Brasel K, Michetti C; AAST Critical Care Committee. Contemporary hemodynamic monitoring, fluid responsiveness, volume optimization, and endpoints of resuscitation: an AAST critical care committee clinical consensus. Trauma Surg Acute Care Open. 2020;5(1):e000411. doi:10.1136/tsaco-2019-000411 Rutherford EJ, Morris JA, Reed GW, Hall KS. Base deficit stratifies mortality and determine therapy. J Trauma. 1992;33(3):417-423. Davis JW, Dirks RC, Kaups KL, Tran P. Base deficit is superior to lactate in trauma. Am J Surg. 2018;215(4):682-683. Jabaley CS, Dudaryk R, Smith CE. Anesthetic considerations and ventilation strategies in cardiothoracic trauma. Curr Anesthesiol Rep. 2016;6:36-49. doi:10.1007/ s40140-016-0149-6 Moran CG, Forward DP. The early management of patients with multiple injuries: an evidence-based, practical guide for the orthopaedic surgeon. J Bone Joint Surg Br. 2012;94(4):446-453. doi:10.1302/0301-620X.94B4.27786 Parent BA, Mandell SP, Maier RV, et al. Safety of minimizing preoperative starvation in critically ill and intubated trauma patients. J Trauma Acute Care Surg. 2016; 80(6):957-963. doi:10.1097/TA.0000000000001011 McClave SA, Taylor BE, Martindale RG, et al; Society of Critical Care Medicine; American Society for Parenteral and Enteral Nutrition. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) CONSID E RAT IONS IN DA M AGE CONT ROL 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr. 2016; 40(2):159-211. doi:10.1177/0148607115621863 Coccolini F, Roberts D, Ansaloni L, et al. The open abdomen in trauma and non-trauma patients: WSES guidelines. World J Emerg Surg. 2018;13:7. doi:10.1186/ s13017-018-0167-4 Polomano RC, Fillman M, Giordano NA, Vallerand AH, Nicely KL, Jungquist CR. Multimodal analgesia for acute postoperative and trauma-related pain. Am J Nurs. 2017;117(3)(suppl 1):S12-S26. doi:10.1097/01. NAJ.0000513527.71934.73 Hayhurst CJ, Pandharipande PP, Hughes CG. Intensive care unit delirium: a review of diagnosis, prevention, and treatment. Anesthesiology. 2016;125(6):1229-1241. doi:10.1097/ALN.0000000000001378 Society of Critical Care Medicine. ICU liberation bundle (A-F). Accessed July 15, 2020. https://www.sccm.org/ ICULiberation/ABCDEF-Bundles Park SY, Lee HB. Prevention and management of delirium in critically ill adult patients in the intensive care unit: a review based on the 2018 PADIS guidelines. Acute Crit Care. 2019;34(2):117-125. doi:10.4266/acc.2019.00451 Hashem MD, Parker AM, Needham DM. Early mobilization and rehabilitation of patients who are critically ill. Chest. 2016;150(3):722-731. doi:10.1016/j.chest.2016. 03.003 Zorowitz RD. ICU-acquired weakness: a rehabilitation perspective of diagnosis, Treatment, and functional management. Chest. 2016;150(4):966-971. doi:10.1016/j. chest.2016.06.006 Coolidge W. Development of a pharmacologic venous thromboembolism protocol for trauma patients. S D Med. 2018;71(10):438-444. Cho MS, Modi P, Sharma S. Transfusion-related acute lung injury. Updated July 26, 2020. Accessed September 6, 2020. https://www.ncbi.nlm.nih.gov/books/NBK507846 Kanat BH, Bozan MB, Emir S, et al. Damage control surgery, actual problems of emergency abdominal surgery. IntechOpen. 2016. doi:10.5772/64326 Smith JW, Matheson PJ, Franklin GA, Harbrecht BG, Richardson JD, Garrison RN. Randomized controlled trial evaluating the efficacy of peritoneal resuscitation in the management of trauma patients undergoing damage control surgery. J Am Coll Surg. 2017;224(4):396-404. Clark E, Edgin R, Emerick M, Joshi M. Infection and infection prevention. In: McQuillan KA, Makic MBF, eds. Trauma Nursing: From Resuscitation through Rehabilitation. 5th ed. Elsevier; 2020:181-228. CE Evaluation Instructions This article has been designated for CE contact hour(s). The evaluation tests your knowledge of the following objectives: 1. Discuss the 3 key components of damage control resuscitation. 2. Describe hemodynamic parameters to assess in patients undergoing damage control resuscitation. 3. Identify the critical care management of patients following damage control surgery including preventing potential complications. Contact hour: 1.0 Synergy CERP Category: A To complete evaluation for CE contact hour(s) for article #ACC3212, visit www.aacnacconline.org and click the “CE Articles” button. No CE evaluation fee for AACN members. This expires on March 15, 2023. The American Association of Critical-Care Nurses is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center’s Commission on Accreditation, ANCC Provider Number 0012. AACN has been approved as a provider of continuing education in nursing by the California Board of Registered Nursing (CA BRN), CA Provider Number CEP1036, for 1.0 contact hour. 75 Copyright of AACN Advanced Critical Care is the property of American Association of Critical-Care Nurses and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.