Rohinton J. Morris, MD
Abington Health Systems
Reasons
Logistics
Process
Results
Abington
Hospital
Reasons
600 bed capacity
Cardiac surgery since 1996 – 3400 cases/year
Two cardiac surgeons
All cases done, except for
transplant
17 & 8 member Cardiology
groups
6 cardiac cath labs
Heart Failure Service
Community of the Elderly
COMPETING FORCES
4 surrounding transplant
centers
22 cardiac surgery centers
in 20 mile radius
Population of 8 million in
surrounding Phila area
Local population of 800K in
primary service area
LOCOREGIONAL NEEDS
15 miles from Philadelphia
Why a VAD program?
Primary Belief:
Service of community – elderly, inadequacy
of HF support
Complementary HF services – to cath lab, EP
service
High-risk cardiac surgery
Satellite to a transplant program
HEART FAILURE
Primary cause of death in
the U.S.
#1 DRG for admissions
Advanced HF is its own
specialty – board
certification by ACC
Demographics of US
population leading
to…greater prevalence of
HF
SURGICAL/CARDIOLOGY
COLLABORATION
Team approach to chronic
disease
Clinicians at front line-but
everybody in hospital
involved – administration,
social work, ER, primary
care, subspecialties.
1.
Better appreciation of
the natural history of
heart failure will improve
outcomes clinically
Treatment options
offered to local
patients
Utilization of resources
efficiently
Earlier recognition of
advanced heart failure
134HTx centers
•
Heart failure, as a specialty, has lagged
significantly behind other areas of cardiology
in diffusing to the community
– CABG
– PCI
– ICD -> Biventricular pacing -> afib ablations
•
Heart failure outcomes in the community are
poor
– 30 day readmission rates up to 25%
– Average LOS nearly 7 days
•
•
Heart failure, as a specialty, has lagged
Hypothesis:
significantly behind
other areas of cardiology
in diffusing to the community
Poor penetration of advanced HF care
– CABG
Poor clinical outcomes
– PCI
– ICD are
-> Biventricular
pacing
-> afibtoablations
driven (largely)
by failure
identify
Heart failure outcomes
stage DinHFthe community are
poor
– 30 day readmission rates up to 25%
– Average LOS nearly 7 days
Logistics
INFRASTRUCTURE
Surgical, cardiologic focus
Special people – VAD
coordinator, HF social
worker
Involvement of multiple
departments- Nutrition,
Phys Ther, echo, ID, Psych,
Administrative belief
EMOTIONAL COMPONENTS
Mission buy-in
Culture of a village
Nursing specialization
Begin w End –goal : Implantation
Work backwards – from Patient identification
Identify team components
Start with basic elements of team
Pt identification
#1
Committee
formation
Basic team members
Simulation – FMEA process
Identify personnel needed
Identify equipment/space/peripherals
What departments are involved? Who needs
education?
What are weak links?
What are likely failure modes?
FAILURE MODE
CHANCE OF OCCURRENCE/EFFECT
– SOLUTIONS??
VAD coordinator sick
Device malfunction
Slow timing of lab results
Lack of blood products
Multiple pt requirements
Operative misadventure
Caregiver stress
Likely/ Moderate
Unlikely/ Drastic
Very likely / Serious
Possible/ Serious
Likely / Mild
(Abstain)/ Serious
Likely/ Moderate
•Mock VAD Implant
•Interdisciplinary team
involvement
•Debriefing after 1st LVAD
implant – 1/24/2012
•Guided by Center for
Patient Safety and
Healthcare Quality
•Maria Wilson & Nancy
McMann
VAD Surgeon(2010)
VAD
Coordinator(2011)
Heart Failure Clinic
Identify
Candidates
Joint Commission
Destination Therapy
Certification
Continued
Program
Growth
FMEA
Establish
Administrative
& Clinical
Committee
1st VAD
Implant
Heart Failure specialist to
start Jan 2013
Process
PRIMARY
ESSENTIAL
Cardiac Surgeon
Heart Failure Cardiologist
VAD coordinator
Social Worker
Heart Failure Nurses
Financial manager
Administrative support
Echocardiographers
Nutritionist
Physical Therapist
Rehab
Outpatient Nursing
Mechanical Cardiac Assist Program –Organizational Structure
Laurence Merlis
President & CEO
Margaret McGoldrick
Executive Vice
President & COO
Marni Guba
Director, Cardiovascular
Service Line
Dr. John J. Kelly
Chief of Staff
Terry O’Reilly
Senior Vice President,
Patient Safety & CNO
Theresa Reilly
Director, Critical care Services
Dr. Richard Eisenstaedt
Chairman, Department of Medicine
Dr. Robert Watson
Chief of Cardiology
Director, Comprehensive Heart
Failure Program
Dr. John Kukora
Chairman, Department of Surgery
To Be Named
Co-Director, CHFP
Medical Director, MCAP
Dr. Rohinton Morris
Chief, Cardiothoracic Surgery
Medical Director, Cardiovascular
Service Line
MCA Program
Kevin Hagan, VAD Coordinator
Education
VAD Inpatient
VAD Outpatient
VAD Committee
•Cardiology
•Cardiac Surgery
•Anesthesia
•Perfusion
•OR Staff
•Nursing
•Social Work/Case Management
•Physical/Occupational/Speech Therapy
•Nutrition
•Finance
•Palliative Care
Performance Improvement
Research
INTERMACS
Chief, Cardiothoracic Surgery
• Home care
Chief of Cardiology
• Rehab
VAD Coordinator
• Anesthesia
HF Nurse Practitioner
• CT Surgery Team – OR RNs, RNFAs, CT
CT Surgeon
NPs
HF Cardiology
Social Work –HF dedicated
• Perfusion
Financial Coordinator
• Pharmacy
Nutrition
Physical/Occup/Speech Therapy • Echocardiography
• Cardiovascular Service Line Director
Palliative Care
• Nursing Administration
HFU, CICU Nursing Staff
CNS (Clin Nurse Spec) Heart Failure• Hospital Senior Leadership
Unit
Critical Care Educator
“We asked each segment to send at least
one designated person to the FMEA
process”
Interdisciplinary team meetings
Operations group meeting – includes
administration
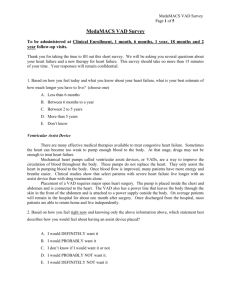
Outpatient VAD Clinic
Combined with Comprehensive Heart Failure Program
Overlap with Aquapheresis Program
Collaboration with multiple transplant centers
Participate in INTERMACS Registry
Majority of patients present via Comprehensive
Heart Failure Program
Major focus on PCP education & referral
Self-referred
Hospital units impacted:
OR
CSU
HFU
ETC
- Cath Lab
- Acute Rehab Unit
Nursing competency
Specialized nursing units: CSU, HFU
Annual unit competencies
New user training class
Sim Lab – in development
Physical & Occupational Therapy competency
Specialized for VAD pt care
Annual requirement
Rehab unit competency
Thoratec online training
Transplant Center
“SHARED CARE”
New Paradigm of care
Greater access of care for
patients
Multiple practice
involvement
Relief on implanting site
for followup care
Revenue sharing
Volume issues / flows
Minor perc site infection
Gout
Fracture in drive line
casing local help from
Thoratec engineer
Acute pulmonary edema
local ER
Routine alarms
Mild anemia
Blood pressure
Profound anemia GIB
Drive line infection with
sepsis
VT + MV endocarditis
ICD generator change
Cataract surgery
Hyperkalemia
Results
Program
growth
--Yearly growth
--Total referrals : 131
--Following 43 patients
--One-year mortality:
9.7%
--Two VAD changeouts
2012
2013
2014
2015
2016
4
12
16
9…
???
IM-1
IM-2
IM-3
IM-4
IM-5
1
17
11
12
0
“Besides payment”
The Mechanical Cardiac Assist Program created a
Performance Improvement (PI) Plan to:
Monitor the process and outcome of patient care
Promote safe, quality and timely provision of care
Improve the knowledge and skills of the MCAP team
Provide the structure that supports performance improvement
The MCAP PI plan is integrated with AMH’s organizationwide PI activities
Patient selection –biggest driver of outcomes
LOS –everybody contributes
Readmission blues
Medical issues
Psychosocial issues
Administration pitfalls
Coding/Billing/Collecting
Staffing
Advanced Heart Failure specialist joined team Jan
2013
Community outreach
Chairman’s Forum
Primary Care Update
Physician outreach / in-reach
Internet promotion
Large DT population in service area – Culture of
the Elderly
September 2011 – Present (Apr 2015):
VAD/Tx Evals: 129
Recommended VAD/Tx: 47
VAD Implants: 46 (41 @ AMH)
TxListed/Potentially Listed (But not VADed): 5
JACC (Jun 2011) – Showed outcomes were no
different in 55 pts that were BTT or DT (split by
age 70) at a 386 bed community hospital
Lead author Robert Adamson –Medical director of
cardiac transplantation program at Sharp
Memorial Hosp, S.D.
Ann Thor Surg – (John, Oct 2011)- PMA study. Compared
outcomes of 486 pts @ 36 centers during clinical
trial, to 1496 pts @ 83 centers posttrial. KaplanMeier survival increased (76 to 85%) in 2nd group.
Presented at AATS-First discussant: “That new VAD
technology that utilizes continuous flow. . .can be
taught along with appropriate patient selection and
disseminated to a broad range of clinical centers.” M.
Acker –Chief of Cardiac Surgery -UPenn
DT is no longer the “future”—It’s here.
More DT/advHF programs are needed for the
community.
A team approach—including hospital
administration & staff– is necessary.
Careful construction, continuous monitoring
and PASSION give great outcomes.
Questions?
 0
0